Intern Ultrasound of the Month: ICD Lead Dislodgment
The Case
A 35-year-old male with severe non-ischemic cardiomyopathy, a recent out-of-hospital cardiac arrest, and a recently implanted implantable cardioverter-defibrillator (ICD) presented to the emergency department with chest pain and palpitations. Recent device interrogation demonstrated loss of right ventricular sensing and capture, raising suspicion for ICD lead dislodgement. Cardiology was consulted, and cardiac point-of-care ultrasound (POCUS) was performed while awaiting their evaluation.
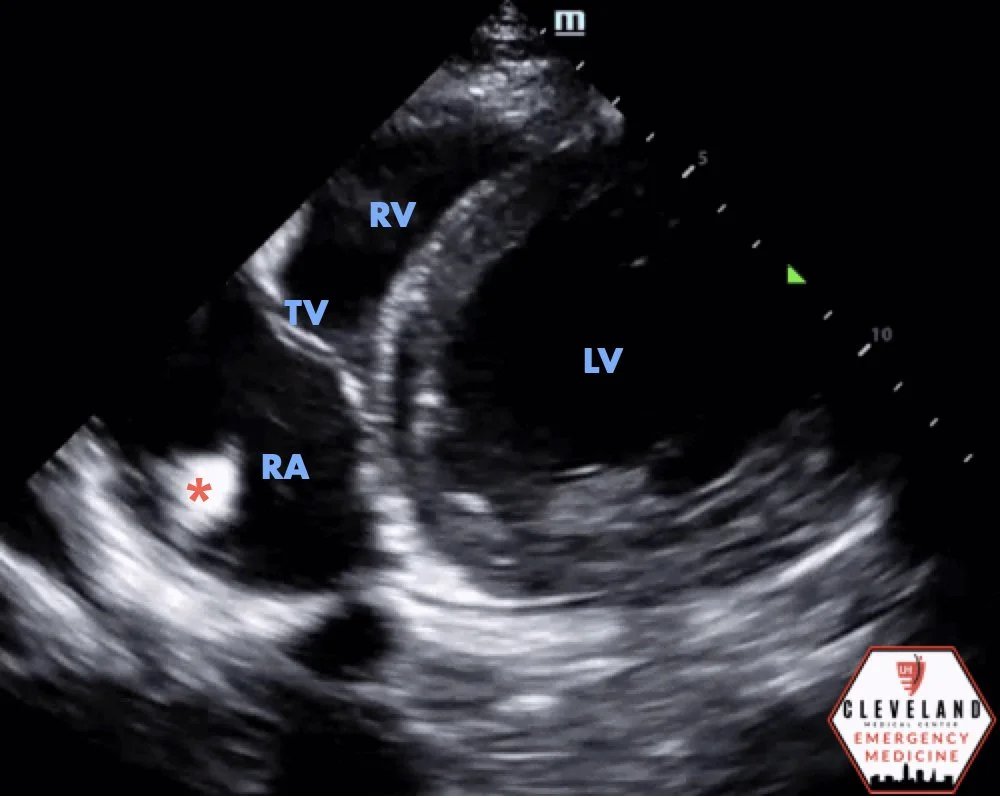
Apical four-chamber view demonstrating the linear ICD lead in the right atrium
Modified parasternal short-axis view
POCUS Findings: Cardiac POCUS revealed a hyperechoic linear structure within the right atrium, rather than its expected position in the right ventricle, concerning for ICD lead dislodgement. The abnormal lead position was confirmed across multiple imaging planes.
Case Conclusion: The combination of POCUS and device interrogation findings confirmed ICD lead dislodgement from the right ventricle into the right atrium. The patient was admitted and underwent successful lead revision the following day, during which his device was upgraded to a left-sided dual-chamber ICD.
Implantable Cardioverter-Defibrillator (ICD) Lead Dislodgement
Introduction
The incidence of implantable cardioverter-defibrillator (ICD) lead dislodgement in contemporary practice is generally reported to be between 1% and 2% for initial implants. In a large registry study of over 20,000 patients, the lead dislodgment event rate was 1.69% per patient and 0.95% per lead over a mean follow-up of 3.3 years, with higher risk in women and those with higher BMI. Data from the National Cardiovascular Data Registry (NCDR) Implantable Cardioverter Defibrillator Registry found an acute lead dislodgment rate of 1.2% (2,628 of 226,764 patients), defined as dislodgment requiring a repeat procedure before hospital discharge (1,2).
ICD lead dislodgment is often first suspected during routine device interrogation, with findings including loss of R-wave sensing, increased pacing thresholds, or failure to capture. These findings should prompt confirmatory imaging with chest radiography, which can reveal an abnormal lead position, or fluoroscopy, which offers real-time assessment (1,2).
In our case, cardiac POCUS played a crucial role in rapidly identifying the abnormal lead position and assessing cardiac anatomy, facilitating timely diagnosis and management.
The Role of Bedside Cardiac Ultrasound in the Emergency Department
This case highlights the value of bedside cardiac POCUS in evaluating patients with suspected ICD malfunction. POCUS enables rapid, dynamic assessment of cardiac anatomy and function at the bedside, allowing emergency physicians to answer focused clinical questions in real time without the delay of formal imaging studies (6,7).
Cardiac POCUS is a versatile tool in the emergency department, offering rapid bedside assessment in a variety of high-acuity scenarios. It is particularly useful in cases of undifferentiated hypotension or shock, where ultrasound can help evaluate for cardiac tamponade, cardiogenic shock, and intravascular volume status. In patients presenting with chest pain or shortness of breath, cardiac POCUS can identify life-threatening conditions such as pericardial effusion, right heart strain from pulmonary embolism, or globally reduced cardiac function (4,6,7).
During cardiac arrest, POCUS can assess cardiac activity, detect tamponade, and evaluate for severely diminished contractility, helping to guide resuscitation efforts. In patients with palpitations or arrhythmias, POCUS may reveal underlying structural abnormalities or provide a rapid assessment of cardiac function. As illustrated in this case, cardiac POCUS can also play an important role in the evaluation of suspected device malfunction, such as confirming the position of an implantable cardioverter-defibrillator (ICD) or pacemaker lead when device interrogation suggests abnormal function (6,7).
Importantly, cardiac POCUS should not be a fishing expedition—it should be guided by a focused clinical question. This ensures that scanning is purposeful, efficient, and interpretable in the clinical context (6,7). Examples of focused questions include: Is there a pericardial effusion? Is left ventricular systolic function reduced? Is the right ventricle dilated? Where is the ICD lead positioned?
In this case, the clinical question was clear: Is the ICD lead properly positioned in the right ventricle? Using apical four-chamber and modified parasternal views focusing on the right heart structures, POCUS demonstrated the lead within the right atrium rather than its expected position in the right ventricle, directly guiding the patient's subsequent admission and intervention.
Patient and Probe Positioning
Optimal cardiac ultrasound imaging begins with proper patient and probe positioning (5,6).
Patient: Ideally, the patient is positioned supine or in the left lateral decubitus position to bring the heart closer to the chest wall, improving image quality in most transthoracic views.
Probe: A phased-array (cardiac) transducer is typically used because its small footprint allows imaging between the ribs while providing adequate depth for cardiac imaging.
Essential Cardiac Ultrasound Views and What You See
Parasternal Long-Axis (PSLA) View
The PSLA view is obtained by placing the probe along the left parasternal border, typically in the 3rd or 4th intercostal space, with the probe marker oriented toward the patient’s right shoulder. This view provides a longitudinal view of the heart and is excellent for assessing global cardiac anatomy and function. Structures visualized include the left ventricle (LV), right ventricle (RV), left atrium (LA), mitral and aortic valves, aortic root, and pericardial space. Clinically, the PSLA view is useful for evaluating LV contractility, RV size, aortic root dilation, and pericardial effusion.
Parasternal Short-Axis (PSSA) View
The PSSA view is obtained by rotating the probe 90° clockwise from the PSLA view so that the marker points toward the patient's left shoulder. This cross-sectional view is particularly useful for evaluating left ventricular wall motion. Depending on the level of imaging, the papillary muscles, mitral valve, or aortic valve may be visualized. The PSSA view is useful for assessing LV wall motion abnormalities, RV dilation, and pericardial effusion.
Apical Four-Chamber (A4C) View
The A4C view is obtained by placing the probe at the cardiac apex, typically near the point of maximal impulse, with the probe marker directed toward the patient's left side. This view allows for simultaneous visualization of all four cardiac chambers and is particularly helpful in evaluating intracardiac relationships. In this case, the A4C view was instrumental in identifying the malpositioned ICD lead within the right atrium rather than its expected location in the right ventricle.
Subxiphoid (Subcostal) View
The subxiphoid view is obtained by placing the probe just below the xiphoid process and angling it superiorly beneath the rib cage toward the heart. It is particularly useful when parasternal or apical views are suboptimal, especially in trauma or critically ill patients. This view is commonly used to evaluate for pericardial effusion, confirm cardiac activity during cardiac arrest, and obtain a general assessment of global cardiac function.
Together, these four views form the foundation of bedside cardiac ultrasound and provide complementary information that guides rapid clinical decision-making (5-7).
Bonus View: Modified Parasternal View Toward Right Ventricular Outflow Tract (RVOT)
In this case, a modified parasternal short-axis view directed slightly toward the right ventricular outflow tract (RVOT) complemented the apical four-chamber view in evaluating the position of the patient's ICD lead. Another common parasternal short-axis imaging plane is the aortic valve level, which provides enhanced visualization of the RVOT, pulmonic valve, and adjacent right-sided cardiac structures, as illustrated in the accompanying labeled image.
Modified parasternal short axis view angled toward RVOT
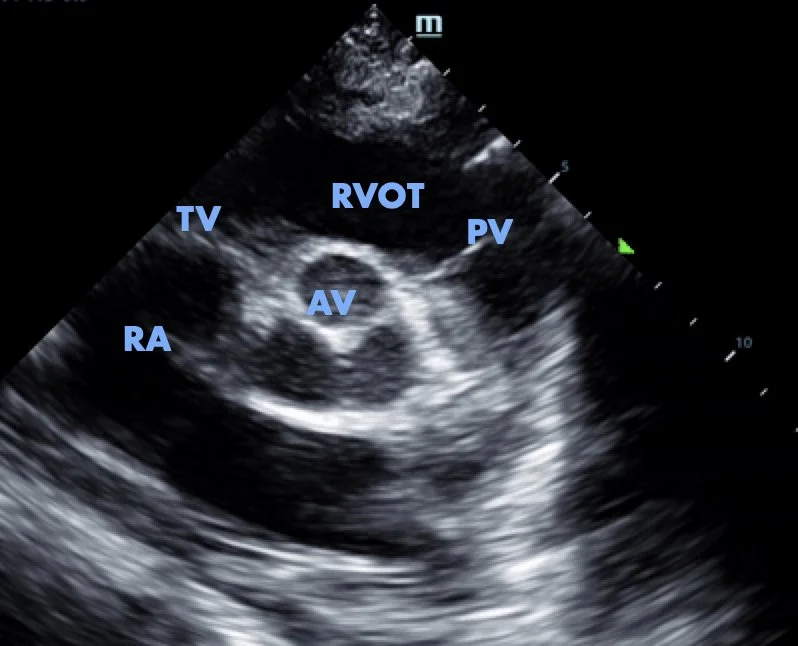
Parasternal short-axis view at the level of the aortic valve, providing enhanced visualization of the RVOT
Key Points
Cardiac POCUS is a rapid bedside tool that helps clinicians answer focused clinical questions in real time.
The core cardiac POCUS views — parasternal long axis, parasternal short axis, apical four-chamber, and subxiphoid — form the foundation of emergency cardiac assessment.
Proper patient positioning and probe selection are essential for obtaining high-quality cardiac images.
The apical four-chamber and RVOT-focused views can be particularly helpful when evaluating suspected ICD lead malposition.
Confirm abnormal findings in multiple imaging planes to improve diagnostic confidence.
In this case, bedside cardiac POCUS rapidly identified ICD lead dislodgement, expediting definitive management.
AUTHORED BY: KYLE COPP, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Qin D, Filippaios A, Murphy J, et al. Short- and long-term risk of lead dislodgement events: real-world experience from Product Surveillance Registry. Circ Arrhythm Electrophysiol. 2022;15(8):e011029.
Cheng A, Wang Y, Curtis JP, Varosy PD. Acute lead dislodgements and in-hospital mortality in patients enrolled in the National Cardiovascular Data Registry Implantable Cardioverter Defibrillator Registry. J Am Coll Cardiol. 2010;56(20):1651-1656.
Młynarski R, et al. Predictors of Early Cardiac Implantable Electronic Device Lead Dislodgement in the Elderly. Int J Environ Res Public Health. 2022;19(22):14766.
Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in Shock in the evaluation of the critically ill. Emerg Med Clin North Am. 2010;28(1):29-56.
POCUS 101. Cardiac Ultrasound (Echocardiography) Made Easy – Step-By-Step Guide. Published February 17, 2021. Accessed July 17, 2025. https://www.pocus101.com/cardiac-ultrasound-echocardiography-made-easy-step-by-step-guide/
American College of Emergency Physicians (ACEP). Policy Statement: Emergency Ultrasound Guidelines. Ann Emerg Med. 2017;69(5):e27-e54.
Vieillard-Baron A, Millington SJ, Sanfilippo F, et al. A decade of progress in critical care echocardiography: a narrative review. Intensive Care Med. 2019;45(6):770-788.