Intern Ultrasound of the Month: DVT
The Case
A 30-year-old female with no significant past medical history presented to the emergency department with several days of progressive right leg pain and swelling. Her only medications were an oral contraceptive pill and a daily multivitamin.
On examination, she had significant edema, erythema, and tenderness extending from the calf to the thigh. Dorsalis pedis and posterior tibial pulses were 2+ bilaterally.
POCUS Findings: The common femoral vein, along with the proximal greater saphenous vein, at the saphenofemoral junction was not compressible, and an occlusive-appearing echogenic clot is visualized within the lumen, consistent with a deep venous thrombosis. The more distal portions of the femoral vein and popliteal veins were compressible.
Case Conclusion: Based on these findings, the patient was started on oral anticoagulation and discharged home.
DVT
Background and Indications
Venous thromboembolism (VTE), including deep venous thrombosis (DVT) and pulmonary embolism (PE), affects approximately 1 in 1,000 individuals annually in the United States. Prompt diagnosis of DVT is essential to prevent complications such as PE, post-thrombotic syndrome, and chronic venous insufficiency (1). Although comprehensive duplex ultrasonography performed by radiology remains the reference standard, access may be limited or delayed in some practice settings because of patient transport requirements, staffing limitations, or after-hours availability, making point-of-care ultrasound (POCUS) a valuable diagnostic adjunct (2).
POCUS, performed at the bedside by emergency physicians, offers a rapid and efficient alternative. Multiple studies have demonstrated that, with appropriate training, emergency physicians can diagnose proximal DVT using compression ultrasonography with high sensitivity and specificity (2-4).
Lower extremity DVT commonly presents with unilateral leg swelling, pain, erythema, warmth, and tenderness. Risk factors include recent surgery, trauma, prolonged immobility, malignancy, pregnancy, estrogen-containing medications, and inherited or acquired hypercoagulable states (2). Clinical decision tools such as the Wells score, combined with D-dimer testing in appropriately selected patients, help determine the need for diagnostic imaging (5).
POCUS is particularly useful in patients with moderate to high pretest probability of DVT, when comprehensive radiology-performed ultrasonography is delayed or unavailable, or when rapid bedside diagnosis may alter immediate management (2).
Image Acquisition
The most widely adopted approach in the emergency department is the three-point compression examination, which evaluates the:
Common femoral vein (CFV), including the saphenofemoral junction (SFJ) and bifurcation into the femoral and deep femoral (profunda femoris) veins
Femoral vein in the proximal to mid-thigh
Popliteal vein (PV) in the popliteal fossa, extending to the trifurcation (2).
While this is the standard emergency department (ED) protocol, it is good practice to follow the common femoral vein distally as it becomes the femoral vein and continues into the popliteal vein, performing compression at the three landmark locations. This systematic approach may improve thrombus detection (2,6).
Earlier two-point compression protocols evaluated only the common femoral and popliteal veins. However, this approach may miss isolated femoral vein thrombosis. In one ED study, 6.3% of patients with suspected DVT had isolated thrombi in proximal venous segments outside the two-point examination, supporting routine evaluation of the femoral vein during compression ultrasonography (7).
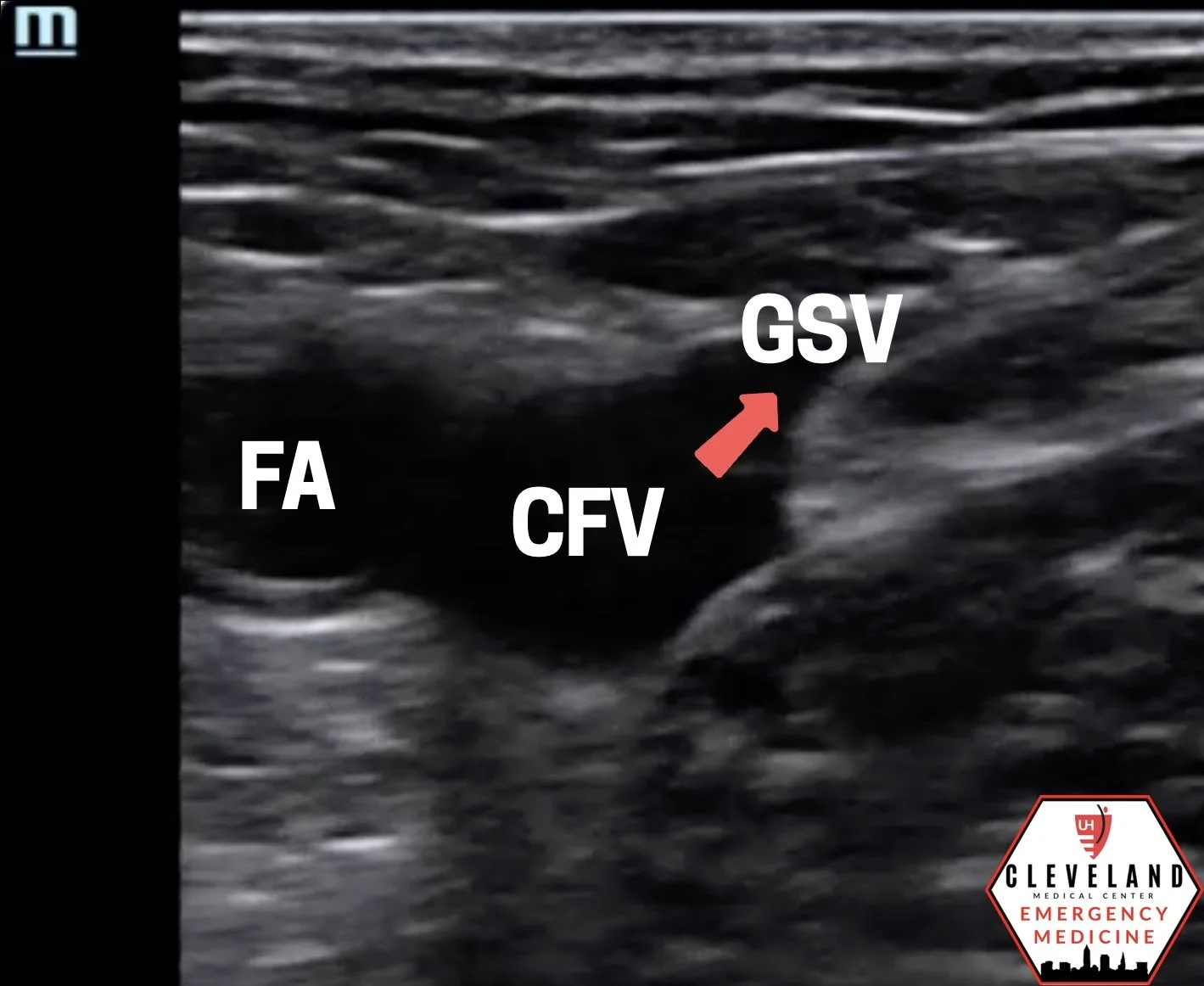
Figure 1. Common femoral vein (CFV) at the saphenofemoral junction, where the great saphenous vein (GSV) joins the common femoral vein medially. FA = femoral artery.
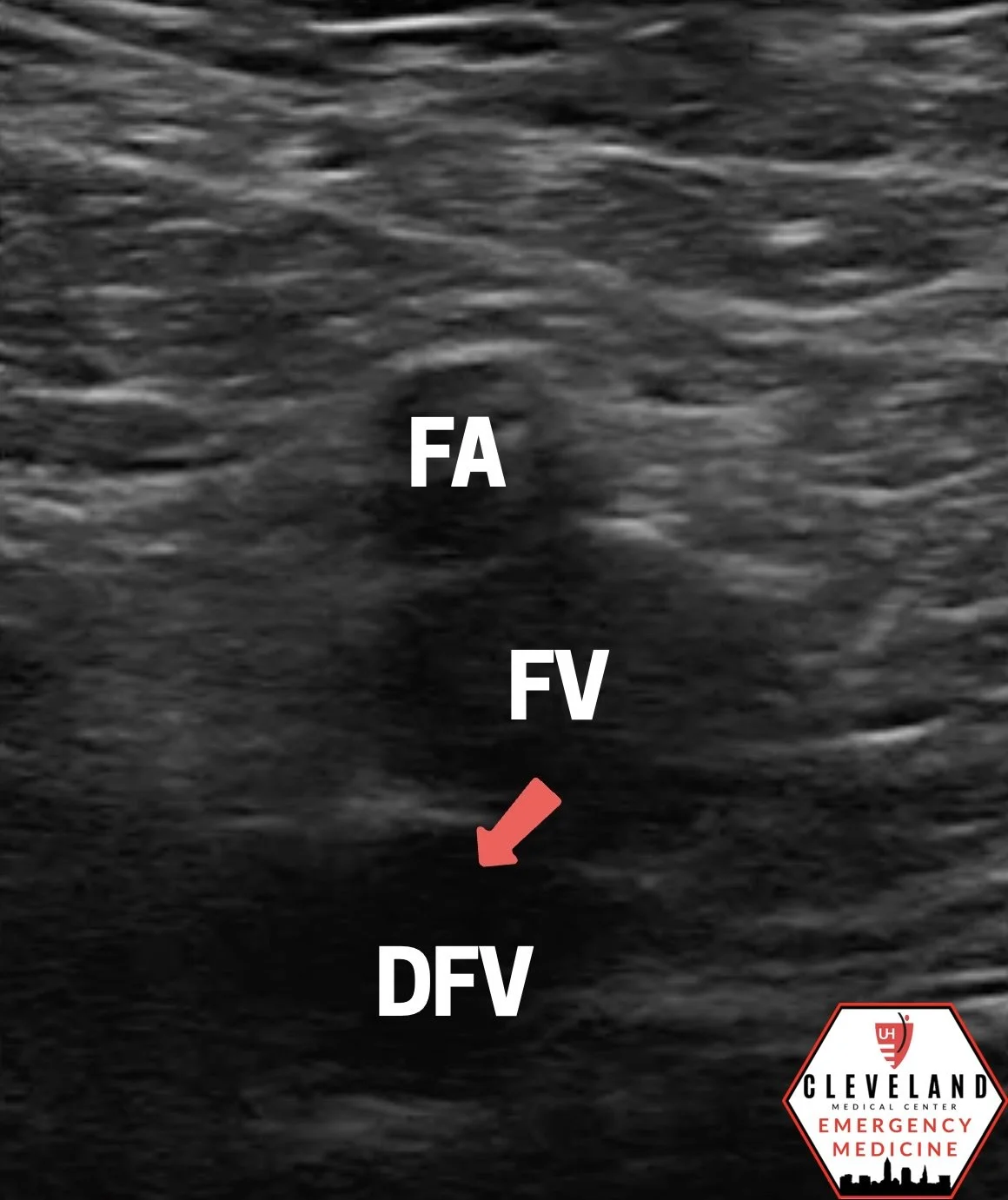
Figure 2. The common femoral vein bifurcates into the femoral vein (FV) and deep femoral vein (DFV).
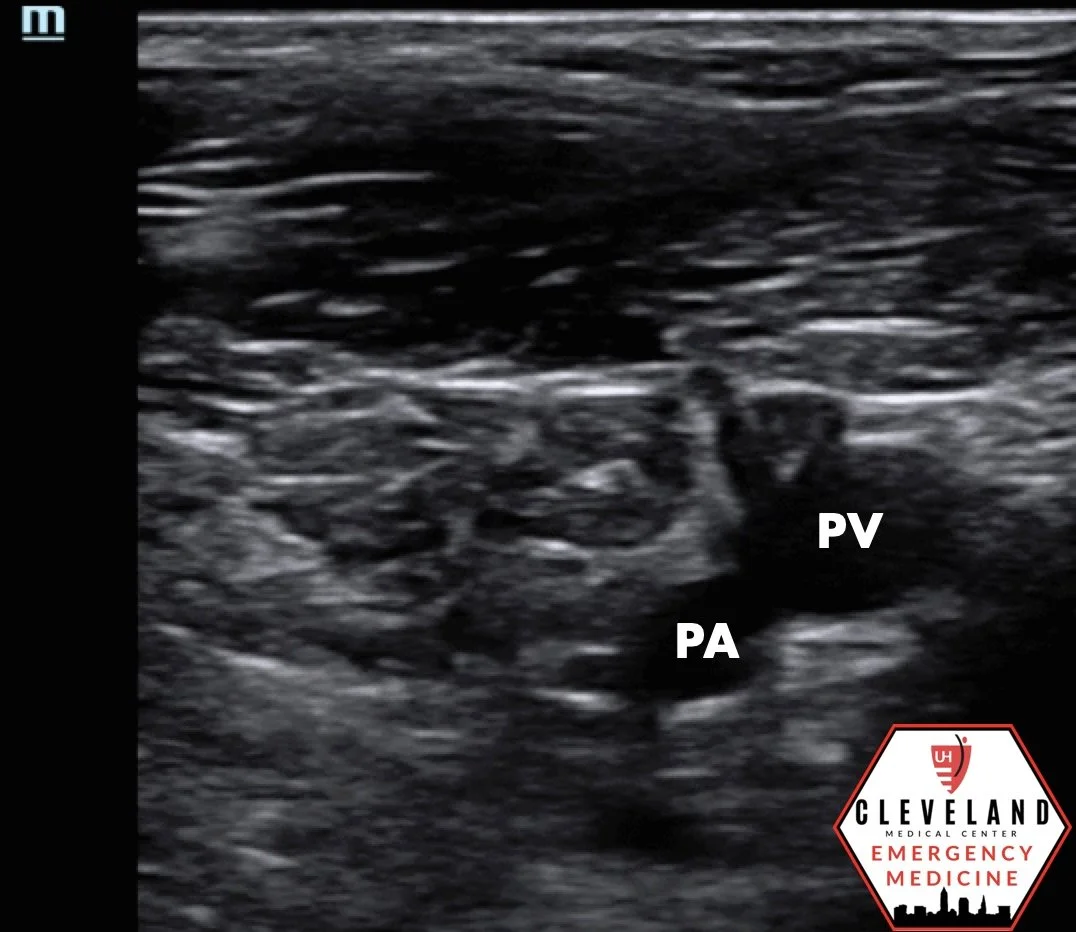
Figure 3. Popliteal vein (PV) superficial to the popliteal artery (PA) in the popliteal fossa. Just distal to this is the trifurcation of the vein (not shown).
Patient Positioning and Equipment
The patient should be positioned supine with the hip externally rotated and the knee slightly flexed. A high-frequency linear transducer (7–12 MHz) is oriented transversely over the vessel. A curvilinear transducer may be helpful in patients with significant edema or obesity (2).
Compression Technique
The examination is performed in the transverse (short-axis) plane. At each location, the probe is pressed perpendicular to the skin to compress the underlying vein. Compression should be performed every 1-2 cm along the course of the vein. A normal vein will completely collapse with gentle probe pressure, while the adjacent artery remains patent. compression. Lack of complete venous compressibility is the hallmark sonographic finding of DVT (2).
Although color or spectral Doppler can provide additional information regarding venous flow, compression ultrasonography alone is sufficient for most ED applications. Doppler may be helpful in equivocal cases or as part of a more comprehensive vascular examination (2).
Interpretation
Positive Findings
Lack of complete venous compressibility (hallmark finding)
Visible intraluminal thrombus
Acute thrombi are often hypoechoic with venous distention, whereas chronic thrombi tend to appear more echogenic and adherent to the vessel wall. Echogenicity alone should not be used to determine thrombus age
Absent or diminished color Doppler flow (if Doppler is used)

Compression ultrasound demonstrating lack of complete venous compressibility, the hallmark sonographic finding of DVT,
Color Doppler demonstrating absent venous flow within a thrombosed vein. Although supportive, Color Doppler is adjunctive to compression ultrasonography in the diagnosis of DVT.
Negative Findings
Complete venous compressibility throughout the examination
Absence of thrombus
Symmetrical venous flow (if Doppler is used (2).
Clinical Significance
POCUS expedites the diagnosis of proximal DVT and may facilitate earlier treatment when appropriate. It is highly accurate for identifying proximal DVT, which carries the greatest risk of PE. Isolated distal calf DVTs may be missed with limited compression protocols; therefore, if clinical suspicion remains high despite a negative examination, formal duplex ultrasonography should be obtained (8).
Emergency physician-performed POCUS has been shown to reduce time to diagnosis while maintaining high diagnostic accuracy, particularly when formal ultrasonography is delayed or unavailable (3,4).
Pearls & Pitfalls
Pearls
Use transverse (short axis) views for optimal compression assessment.
Compress the vein every 1-2 cm rather than relying solely on compression at landmark locations.
Identify arteries by their pulsatility to avoid mistaking them for veins.
A curvilinear transducer may improve visualization in patients with significant edema or obesity (2).
Pitfalls
Mistaking lymph nodes, Baker cysts, or arteries for thrombosed veins.
Applying inadequate probe pressure, resulting in incomplete venous compression.
Mistaking chronic post-thrombotic changes for acute DVT (2).
Limiting the examination to only the common femoral and popliteal veins, potentially missing isolated femoral vein thrombosis (2,7).
Failing to recognize duplicated femoral veins, which may result in a missed DVT (2).
Take Home Points
Lack of complete venous compressibility is the hallmark sonographic finding of DVT.
Systematically follow the femoral vein rather than relying solely on three-point compression.
POCUS is highly accurate for proximal DVT but less sensitive for isolated distal calf thrombosis.
If POCUS is negative but clinical suspicion remains high, obtain formal duplex ultrasonography.
AUTHORED BY: SUELA LAMAJ, MD
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol. 2015;12(8):464–474.
Schafer JM, Stickles S. Deep Vein Thrombosis (DVT). ACEP Sonoguide. American College of Emergency Physicians. Updated August 18, 2020. Available from: https://www.acep.org/sonoguide/basic/dvt
Frazee BW, Snoey ER, Levitt A. Emergency department compression ultrasound to diagnose proximal deep vein thrombosis. Ann Emerg Med. 2010;56(6):601-610.
Burnside PR, Brown MD, Kline JA. Systematic review of emergency physician-performed ultrasonography for lower-extremity deep vein thrombosis. Acad Emerg Med. 2008;15(6):493–498.
Bates SM, Jaeschke R, Stevens SM, et al. Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e351S-e418S
Maki DD, Kumar N, Nguyen B, Langer JE, Miller WT Jr, Gefter WB. Distribution of thrombi in acute lower extremity deep venous thrombosis: implications for sonography and CT and MR venography. AJR Am J Roentgenol. 2000;175(5):1299-1301.
Adhikari S, Zeger W, Thom C, Fields JM. Isolated deep venous thrombosis: implications for 2-point compression ultrasonography of the lower extremity. Ann Emerg Med. 2015;66(3):262-266.
Bernardi E, Camporese G, Buller HR, et al. Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasound for diagnosing suspected deep vein thrombosis: a randomized controlled trial. JAMA. 2008;300(14):1653–1659.