Intern Ultrasound of the Month: Posterior Vitreous Detachment
The Case
60-year-old female with a history of remote LASIK surgery presented to the emergency department (ED) with two days of painless floaters in her left eye. She described the sudden onset of a “galaxy-shaped” circular floater in the center of her left visual field. She also noted surrounding "dust-like" floaters. The floater was intermittent and disappeared when looking directly at it. She denied recent trauma, a family history of retinal detachment, or prior retinal disease.
On exam, visual acuity was 20/20 in each eye and extraocular movements were intact.
Ocular point-of-care ultrasound (POCUS) was performed to evaluate for retinal detachment, posterior vitreous detachment, and vitreous hemorrhage as potential causes of her painless visual symptoms.

Figure 1. Fanning through the globe in transverse orientation
Figure 2. Transverse oculokinetic views
POCUS Findings: There was a thin, mobile hyperechoic membrane within the posterior vitreous that crossed the optic nerve without remaining tethered to it, consistent with posterior vitreous detachment. During the oculokinetic exam, the membrane moved freely with increased echogenicity between the detached vitreous and posterior globe. No sonographic evidence of retinal detachment was identified.
Case Conclusion: Ophthalmology was consulted and confirmed the diagnosis of posterior vitreous detachment, along with associated retinal tears. Because retinal tears significantly increased the risk of subsequent retinal detachment, urgent laser retinopexy was performed in the ED. The patient tolerated the procedure well and was discharged home with ophthalmology follow-up in 1-2 weeks.
Posterior Vitreous Detachment
Pathophysiology & Clinical Significance
Posterior Vitreous Detachment (PVD) is the most common cause of floaters and is defined as the separation of the posterior vitreous cortex and the internal limiting membrane of the retina (1). The vitreous matrix or gel is normally adherent to the retina. With aging, it gradually liquefies and contracts, eventually separating from the retinal surface. This separation is referred to as PVD and can produce floaters and flashes as the detached vitreous casts shadows onto the retina (1).
Although the diagnosis is typically confirmed by dilated fundoscopic and slit-lamp examination, ocular POCUS is a useful bedside adjunct that can help differentiate PVD from retinal detachment and vitreous hemorrhage in the emergency department (2).
Management of PVD without associated vitreous hemorrhage or retinal tears is generally conservative. However, when PVD is associated with retinal tears, as in this case, approximately 50% of acute symptomatic retinal tears with persistent vitreoretinal traction progress to retinal detachment if left untreated. Laser retinopexy is typically performed under topical anesthesia and involves creating small laser burns around the retinal tear. These burns stimulate scar tissue formation, creating a “weld” that seals the tear and helps prevent progression to retinal detachment (3,4).
Ocular Point-of-Care Ultrasound
Indications
Acute painless vision loss or visual disturbance
Floaters or flashes
Ocular trauma
Eye pain when posterior pathology is suspected
Evaluation of optic nerve sheath diameter when elevated ICP is suspected (5)
Contraindications
Suspected globe rupture — avoid ultrasound, as even minimal pressure may worsen ocular injury. CT imaging should be obtained instead (5)
Materials:
High-frequency linear transducer
Tegaderm dressing
Ultrasound gel
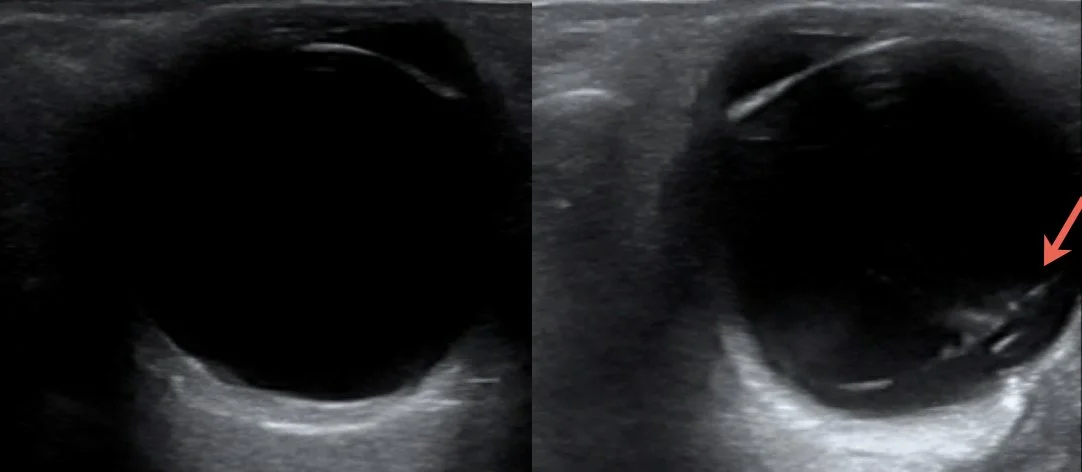
Figure 2. Comparison of standard gain (left) and increased gain (right), demonstrating improved visualization of posterior vitreous detachment with higher gain settings.
Technique for Ocular Ultrasound
Position the patient with the head of the bed elevated to approximately 45°. Place a large Tegaderm dressing over the closed eyelid and apply copious ultrasound gel.
Using a high-frequency linear transducer and minimal pressure, gently scan the eye in both the sagittal and transverse planes (5).
Ensure the vitreous body, retina, and optic nerve are clearly visualized. Identifying the optic nerve is particularly important when differentiating posterior vitreous detachment from retinal detachment (Figures 2 and 4). (5,6)
Start with standard gain, and slowly increase gain to improve visualization of posterior vitreous pathology, including PVD, retinal detachment, and vitreous hemorrhage (Figure 3) (7).
Perform a dynamic (oculokinetic) examination by asking the patient to look left and right (transverse orientation) and up and down (sagittal orientation) while maintaining the probe position. Dynamic imaging can improve visualization and help distinguish posterior ocular pathologies (Figure 1) (5,6).
Consider imaging the contralateral eye for comparison (5).
Distinguishing Posterior Ocular Pathologies
PVD appears as a thin, mobile hyperechoic membrane that is not attached to the optic nerve and may cross the optic disc during static or dynamic examination (Figure 3). In contrast, retinal detachment remains tethered to the optic nerve and represents an ophthalmologic emergency requiring urgent consultation. Vitreous hemorrhage appears as mobile echogenic debris within the vitreous rather than a discrete membrane. Recognizing these distinguishing features can improve diagnostic accuracy and help prioritize ophthalmologic evaluation (Figure 4) (2,4,6).
Although ocular POCUS can distinguish PVD from retinal detachment, retinal tears are generally not visualized sonographically. Patients with acute symptomatic PVD should therefore undergo ophthalmologic evaluation even in the absence of sonographic retinal detachment (3,4).
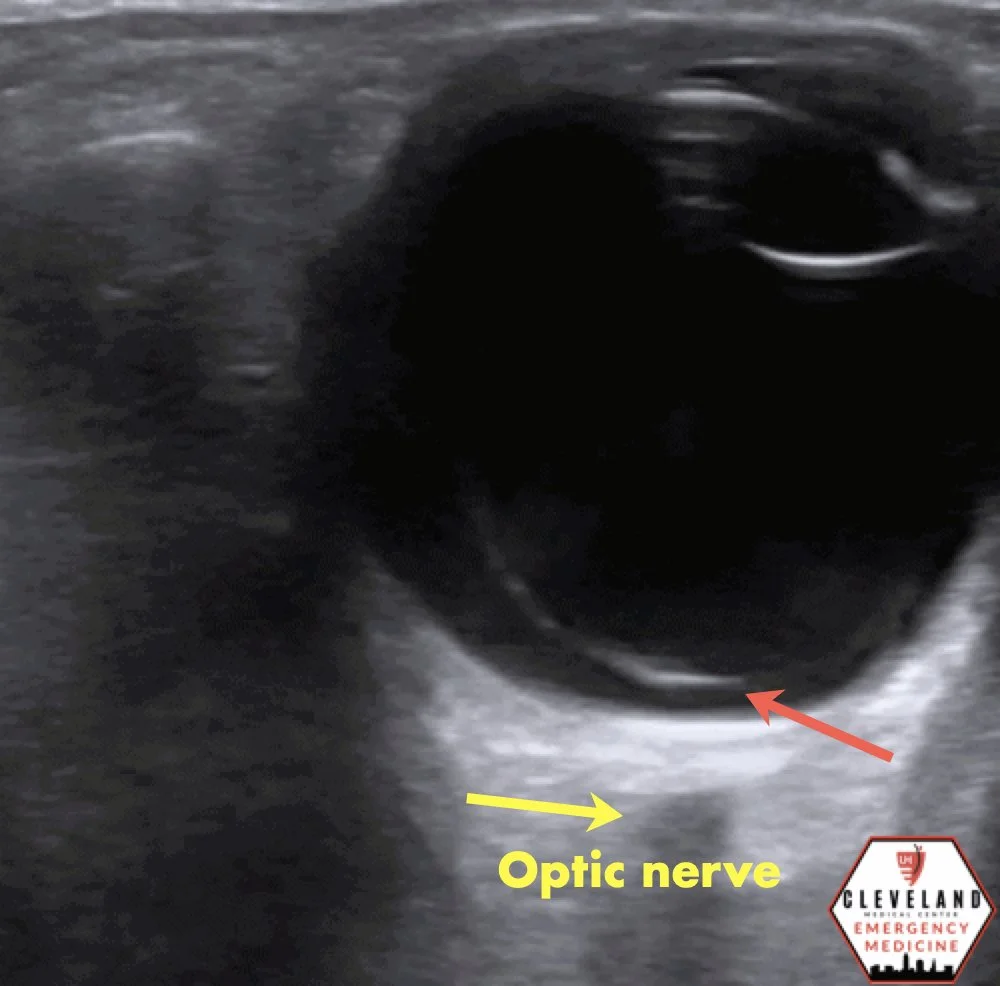
Figure 3. PVD crossing midline and over the optic nerve
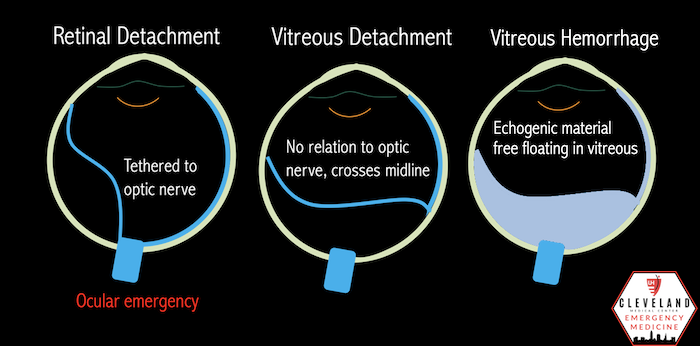
Figure 4. Illustration differentiating common posterior ocular pathologies with POCUS
Take Home Points
Ocular POCUS is a valuable bedside adjunct that can rapidly differentiate common posterior ocular pathologies, but it does not replace a comprehensive ophthalmologic examination.
Consider ocular ultrasound in patients with acute painless vision changes, including floaters, flashes, or vision loss, unless an open globe injury is suspected.
Using a consistent scanning technique—including adequate gain and dynamic oculokinetic examination—improves visualization of posterior ocular pathology.
PVD appears as a thin, mobile hyperechoic membrane that is not attached to the optic nerve and may cross the optic nerve during dynamic examination.
Retinal detachment remains tethered to the optic nerve and is an ophthalmologic emergency. Among common posterior chamber abnormalities, ocular POCUS has the highest diagnostic accuracy for retinal detachment.
Ocular ultrasound does not replace a comprehensive ophthalmologic exam but can expedite the diagnosis, help determine the urgency of ophthalmology evaluation, and is a readily learned bedside skill.
AUTHORED BY: MARCO LORICO-RAPPA, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Ahmed F, Tripathy K. Posterior vitreous detachment. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated August 25, 2023. Accessed January 2025.
Fincham GS, James S, Spickett C, et al. Posterior vitreous detachment and the posterior hyaloid membrane. Ophthalmology. 2018;125(2):227-236.
Flaxel CJ, Adelman RA, Bailey ST, et al. Posterior vitreous detachment, retinal breaks, and lattice degeneration preferred practice pattern. Ophthalmology. 2020;127(1):P146-P181.
Propst SL, Kirschner JM, Strachan CC, et al. Ocular point-of-care ultrasonography to diagnose posterior chamber abnormalities: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(2):e1921460.
Ocular ultrasound. Core EM. https://coreem.net/core/ocular-ultrasound/
Vrablik ME, Snead GR, Minnigan H, et al. The diagnostic accuracy of bedside ocular ultrasonography for the diagnosis of retinal detachment: a systematic review and meta-analysis. Ann Emerg Med. 2015;65(2):199-203.e1.
Chang M, Finney N, Baker J, et al. Optimal image gain intensity of point-of-care ultrasound when screening for ocular abnormalities in the emergency department. West J Emerg Med. 2023;24(3):622-628.