Intern Ultrasound of the Month: Detection of Aortic Dissection During Cardiac Arrest
The Case
A 50-year-old male with an unknown past medical history presented to the emergency department in cardiac arrest after being found unresponsive by family. EMS reported a persistent non-shockable rhythm from initial contact through transport. Point-of-care ultrasound (POCUS) was performed during resuscitation to evaluate for reversible causes of cardiac arrest. Initial venous blood gas analysis demonstrated a profound metabolic acidosis with markedly elevated lactate.
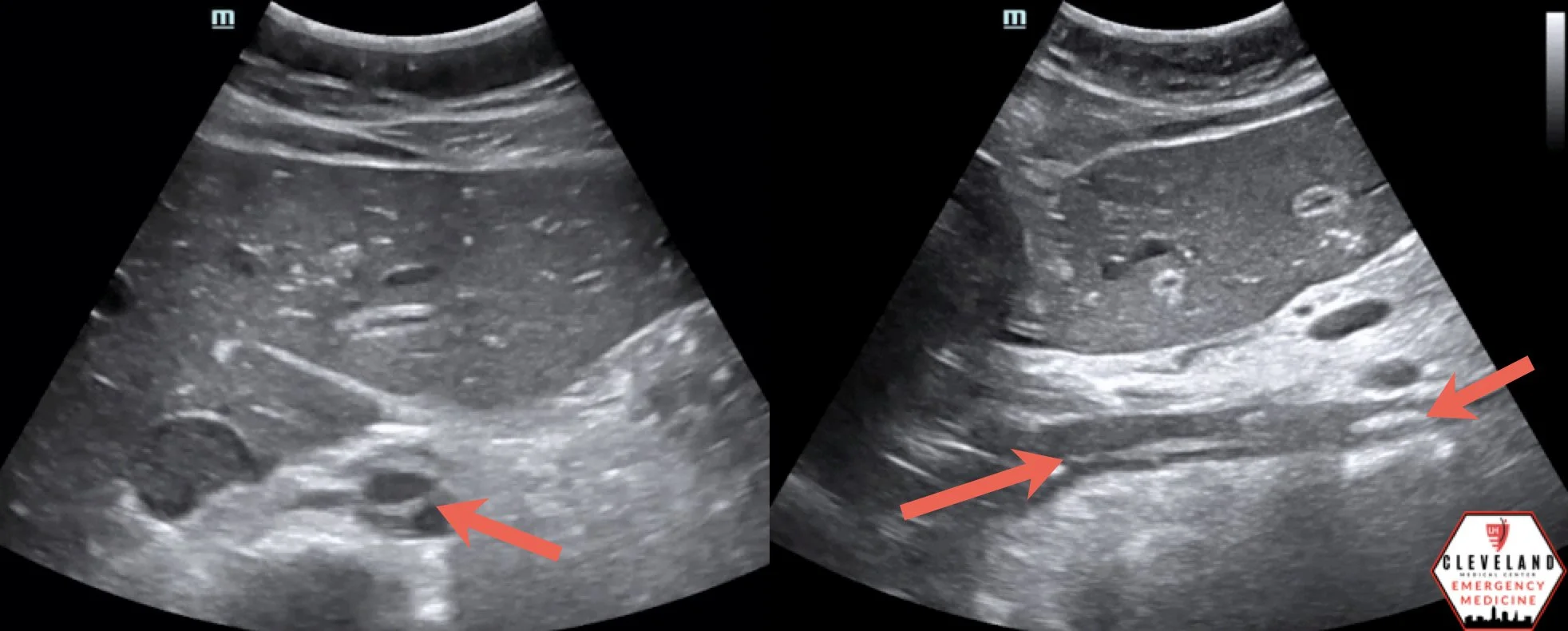
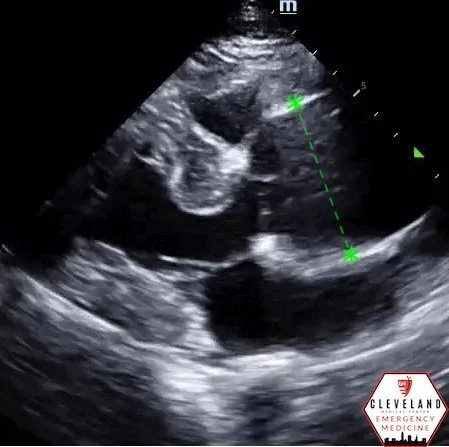
The parasternal long-axis view demonstrated cardiac standstill and a large pericardial effusion with a normal-appearing aortic root. Given concern for cardiac tamponade as a potentially reversible cause of the arrest, emergent pericardiocentesis was performed without return of spontaneous circulation. Resuscitation continued, including further POCUS evaluation of the abdominal aorta, which revealed an intimal flap consistent with acute aortic dissection. In the setting of ongoing resuscitation and these catastrophic findings, efforts were terminated.
This case highlights the value of incorporating POCUS into cardiac arrest resuscitation—not only to assess cardiac activity and reversible causes of arrest, but also to identify catastrophic aortic pathology that can rapidly guide diagnosis and management.
Why POCUS in Cardiac Arrest?
POCUS is an invaluable tool during cardiac arrest and peri-arrest resuscitation, providing rapid bedside diagnostic information that can be obtained during pulse checks while minimizing interruptions in chest compressions. It allows clinicians to assess for cardiac activity and identify potentially reversible causes of arrest, including right heart strain suggestive of pulmonary embolism, pericardial effusion with tamponade physiology, tension pneumothorax, intra-peritoneal free fluid concerning for hemorrhage, hypovolemia, and acute aortic pathology. (1-3)
POCUS can also differentiate true asystole from fine ventricular fibrillation, as subtle, rapid myocardial quivering may be visualized on ultrasound even when the EKG appears flat, potentially prompting appropriate defibrillation (4).
When acute aortic syndromes are on the differential, POCUS may also identify direct and indirect signs of aortic dissection. These include visualization of an intimal flap, dilation of the aortic root or ascending aorta, new aortic regurgitation, and pericardial effusion—findings that raise concern for proximal (Type A) dissection and tamponade physiology (1,2,5).
During cardiac arrest, POCUS can be incorporated as part of a focused Rapid Ultrasound for Shock and Hypotension (RUSH)-style evaluation, providing a structured approach to assessing for catastrophic and potentially reversible causes of arrest (6).
Assessment for Aortic Dissection using POCUS
Aortic dissection is an uncommon but highly lethal diagnosis with clinical presentations that often mimic other conditions. It results from disruption of the medial layer of the aorta, typically secondary to an intimal tear that may be visualized on ultrasound. Mortality for Type A dissections increases by approximately 1–2% per hour during the first 24–48 hours, underscoring the time-sensitive nature of diagnosis (1,7,8).
Computed tomography angiography (CTA) remains the gold standard for diagnosis, with reported sensitivity approaching 100% and specificity of approximately 98% (2,7). However, unstable patients may not tolerate transport or delays to advanced imaging. In this context, POCUS serves as a valuable bedside screening tool.
The Sonographic Protocol for the Emergent Evaluation of Aortic Dissections (SPEED) demonstrated a sensitivity of 93.2% and specificity of 90.9% for the detection of aortic dissection using a combination of transthoracic echocardiography (TTE) and abdominal aortic ultrasound (2). Direct visualization of an intimal flap is diagnostic, while indirect findings, including a dilated left ventricular outflow tract (>35 mm) and pericardial effusion, improve the sensitivity of the examination (2,9).
Additionally, a recent study found that more than one in seven patients with a dilated aortic root identified on POCUS (defined as aortic root diameter >45 mm) were found to have an associated thoracic aortic dissection (10).
The presence of a pericardial effusion or hemothorax on POCUS in the setting of suspected aortic dissection is concerning for impending or active rupture and carries a poor prognosis (8,9).
Prehospital POCUS: An Emerging Role
Given the time-dependent mortality of aortic dissection, early diagnosis is critical. Prehospital POCUS may facilitate earlier recognition and expedite definitive care. A recent case report from Italy described prehospital identification of a dilated aortic root with an intimal flap and small pericardial effusion, prompting transport to a facility with cardiothoracic surgery capabilities and resulting in a favorable outcome (11).
More broadly, POCUS can meaningfully alter a patient’s clinical trajectory in both critically ill patients and cardiac arrest by expediting advanced imaging, mobilizing consultants, and providing actionable diagnostic information. A focused cardiac examination that includes assessment of the abdominal aorta can narrow the differential diagnosis and improve time to definitive care (3).
Ultrasound Evaluation: Practical Approach
Aortic Root and Aortic Regurgitation
The aortic root is best measured in the parasternal long-axis view at end-diastole using a leading-edge to leading-edge technique just above the aortic valve (8,9). When measuring the aortic annulus, an inner edge–to–inner edge measurement obtained during mid-systole is recommended (9). As a general rule of thumb for POCUS, an aortic root diameter ≤4.0 cm is considered normal, with values approaching or exceeding this threshold concerning for dilation (8).
Color Doppler can be used to assess for aortic regurgitation during diastole (9). When evaluating the root, care should be taken not to confuse normal aortic valve leaflets with an intimal flap (8).
Pericardial Effusion
Pericardial effusions are most commonly visualized in the parasternal long-axis or subxiphoid views. The parasternal long-axis view is particularly helpful, as it allows differentiation between pericardial and pleural effusions. A pericardial effusion appears as an anechoic stripe between the posterior wall of the heart and the descending thoracic aorta, helping distinguish it from a pleural effusion, which lies posterior to the descending aorta (9).
Identification of an Intimal Flap
An intimal flap divides the aorta into true and false lumens. Multiple views can be used to assess different segments of the aorta:
Parasternal long-axis: Ascending and descending thoracic aorta
Apical four-chamber: Descending thoracic aorta
Subcostal view: Abdominal aorta
Suprasternal notch view: Aortic arch and supra-aortic vessels — This view is obtained by placing the probe in the suprasternal notch and directing it toward the patient’s chest to visualize the arch (9)
When evaluating the abdominal aorta, begin in the subcostal window by identifying the inferior vena cava and aorta, then slide the probe distally and rotate it to visualize the aorta in both short- and long-axis planes.
POCUS Pearls During Cardiac Arrest
Position the probe before the pulse check to facilitate rapid image acquisition.
Save cine clips during pulse checks, resume compressions immediately, and interpret images while compressions continue to minimize hands-off time.
During active chest compressions, complete other components of a RUSH-style evaluation to assess for potential causes of arrest (6).
Incorporate ultrasound early when evaluating critically ill patients and those in cardiac arrest, as early imaging can meaningfully narrow the differential and expedite definitive care (3,5).
Key Takeaway
POCUS is a powerful adjunct during cardiac arrest, enabling clinicians to rapidly evaluate for reversible and catastrophic causes of arrest. Although aortic root dilation is an important clue to proximal aortic dissection, a normal-appearing aortic root does not exclude the diagnosis. Extending the examination to include the abdominal aorta may reveal an intimal flap and provide critical diagnostic information that influences time-sensitive clinical decision-making.
AUTHORED BY: JOANNA DEHGHANI, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191–196.
Gibbons RC, Smith D, Feig R, Mulflur M, Costantino TG. The sonographic protocol for the emergent evaluation of aortic dissections (SPEED protocol): a multicenter, prospective, observational study. Acad Emerg Med. 2024;31(2):112–118.
Pare JR, Liu R, Moore CL, Sherban T, Kelleher MS Jr, Thomas S, Taylor RA. Emergency physician–focused cardiac ultrasound improves diagnosis of ascending aortic dissection. Am J Emerg Med. 2016;34(3):486–492.
Gaspari R, Adhikari S, Gleeson T, et al. Occult Ventricular Fibrillation Visualized by Echocardiogram During Cardiac Arrest: A Retrospective Observational Study From the Real-Time Evaluation and Assessment for Sonography-Outcomes Network (REASON). JACEP Open. 2025;6(1):100028.
Gibbons R, Smith D, Mulflur M, Dai T, Satz W, Goett H, et al. Point-of-care ultrasound for the detection of aortic dissections in the emergency department. Ann Emerg Med. 2017;70(suppl 1):S143.
Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically ill. Emerg Med Clin North Am. 2010;28(1):29-56.
Meredith EL, Masani ND. Echocardiography in the emergency assessment of acute aortic syndromes. Eur J Echocardiogr. 2009;10(1):i31-i39.
Liu F, Huang L. Usefulness of ultrasound in the management of aortic dissection. Rev Cardiovasc Med. 2018;19(3):103-109.
Evangelista A, Flachskampf FA, Erbel R, Antonini-Canterin F, Vlachopoulos C, Rocchi G, et al. Echocardiography in aortic diseases: EAE recommendations for clinical practice. Eur J Echocardiogr. 2010;11(8):645–658.
Hesami M, Denkewicz R, Boivin Z, Bhalodkar S, Li JJ, Moore C. Association of dilated aortic root on point-of-care ultrasound with aortic aneurysm and dissection. Am J Emerg Med. 2025;95:89–94.
Ripoll-Gallardo A, Cabrini M, Cairo M, Mori A, Diana V, Boschiroli P, et al. A case report of prehospital point-of-care ultrasound in acute aortic dissection: reinforcing the out-of-hospital chain of survival. Prehosp Emerg Care. 2025;29(1):1-6.