Intern Ultrasound of the Month: Left Atrial Mass vs Thrombus
The Case
An elderly female presented to the emergency department with altered mental status and decreased responsiveness per her family. She had told her family she didn’t feel well earlier in the day, and a few hours later, they found her unresponsive to verbal and tactile stimuli.
On exam, she was tachycardic but hemodynamically stable. She did not open her eyes, produce verbal responses, or withdraw to painful stimuli. Her Glasgow Coma Scale (GCS) was 3. She was intubated for airway protection and underwent emergent CT imaging, which revealed multiple infarcts involving not only the brain as well as multiple abdominal organs.
Given concern for a central embolic source, cardiac point-of-care ultrasound (POCUS) was performed.
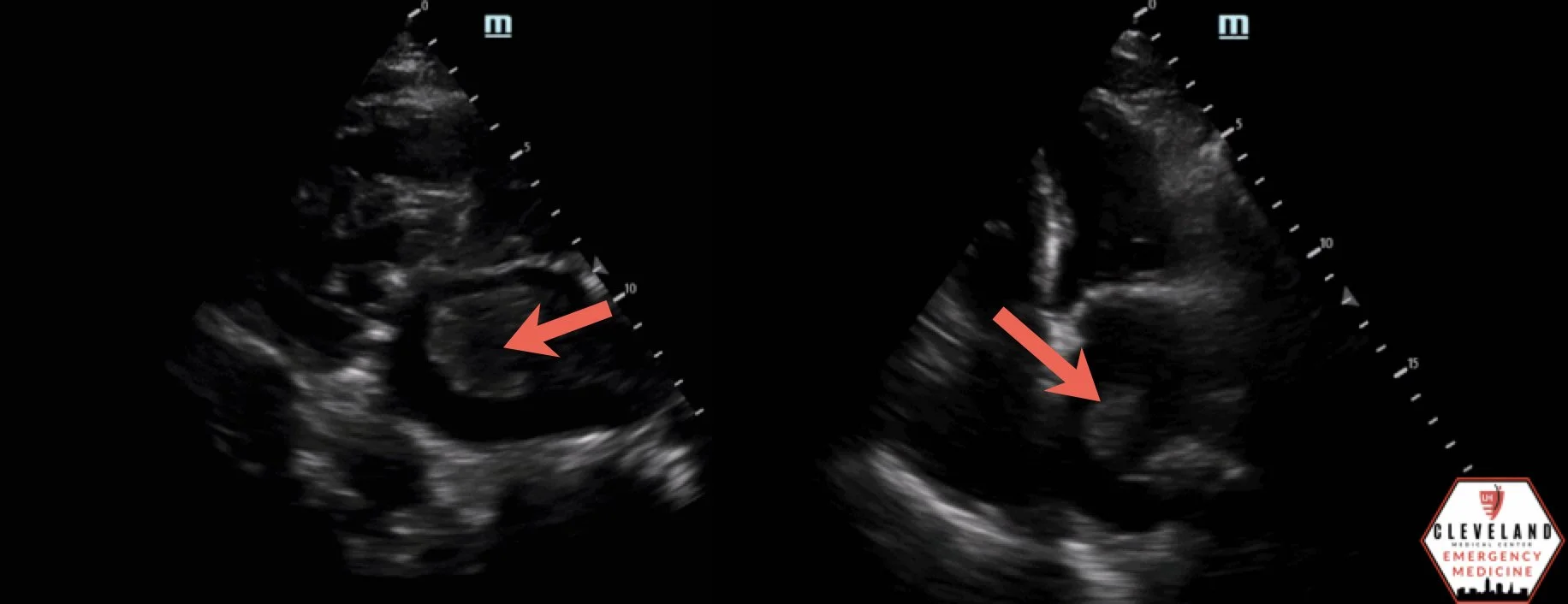
POCUS Findings: Focused cardiac ultrasound demonstrated a large, mobile echogenic mass within the left atrium, concerning for either an atrial thrombus or cardiac myxoma.
Case Conclusion: POCUS findings were suggestive of a large left atrial mass, but imaging alone could not determine whether it represented a thrombus, myxoma, or a combination of both. Given the patient's extensive multiorgan embolic infarcts, thrombus was strongly suspected. Further chart review revealed multiple risk factors for thrombus formation and a previously documented left atrial mass versus thrombus that had not undergone definitive evaluation.
Cardiac Myxoma and Atrial Thrombus
The most common primary cardiac tumor is the atrial myxoma, with most arising from the interatrial septum of the left atrium (1, 2). Myxomas vary in appearance and may be smooth, polypoid, villous, or friable. Villous and irregular myxomas are associated with a higher risk of embolization, whereas smooth myxomas are more likely to present with obstructive symptoms depending on their size and location (1).
Left atrial thrombi most commonly originate within the left atrial appendage and develop in conditions that promote blood stasis, particularly atrial fibrillation (3,4). Other important risk factors include mitral valve disease, rheumatic heart disease, and hypercoagulable states (1, 3). Irregular intracardiac structures, including myxomas, may also serve as a nidus for thrombus formation (2).
Clinical Significance
Both atrial myxomas and left atrial thrombi are important causes of systemic embolization. Patients may present with ischemic stroke, but emboli can also affect the kidneys, spleen, liver, and other organs, as demonstrated in this case (1, 2). Recognition of multiorgan infarction should prompt consideration of a central embolic source and early cardiac imaging.
Imaging Considerations
Transthoracic echocardiography (TTE), including point-of-care ultrasound (POCUS), can rapidly identify intracardiac masses at the bedside, making it a valuable first-line modality in the emergency department. However, TTE is less sensitive than transesophageal echocardiography (TEE), particularly for evaluating the left atrial appendage and characterizing left atrial masses (3,4). While POCUS can identify abnormal intracardiac pathology and raise suspicion for a cardiac source of embolization, it often cannot reliably distinguish thrombus from myxoma or other cardiac tumors. Definitive diagnosis may require advanced imaging and, in some cases, histopathologic evaluation (2).
POCUS Practical Application and Pattern Recognition
Although distinguishing atrial thrombus from myxoma can be challenging on transthoracic imaging alone, POCUS remains a powerful bedside tool for rapidly identifying large intracardiac masses and raising suspicion for a cardiac source of systemic embolization (5).
Certain imaging features may help narrow the differential. Myxomas are often mobile and pedunculated with irregular or villous morphology, whereas thrombi tend to appear more layered, sessile, or less mobile. However, there is considerable overlap in appearance, and these findings should be interpreted within the clinical context (2).
In the emergency department, recognition of an intracardiac mass on POCUS can expedite specialty consultation, definitive cardiac imaging, and appropriate management, even when the exact diagnosis remains uncertain.
Technique and View Selection
A complete four-view cardiac POCUS examination should be performed whenever intracardiac pathology is suspected, as masses may not be equally visible in every view (6,7).
Parasternal Long Axis: Useful for identifying left atrial pathology and evaluating the relationship of a mass to the mitral valve and left ventricular inflow. (6,7).
Parasternal Short Axis: Primarily assesses ventricular size and function but may provide additional information with slight probe adjustments toward the mitral valve (6,7).
Apical Four-Chamber: Often provides the best visualization of left atrial masses, allowing assessment of size, mobility, and relationship with the mitral valve. (4,5,7).
Subxiphoid Four-Chamber: Offers an alternative four-chamber view when parasternal or apical windows are limited and can help confirm intracardiac pathology (6,7)
POCUS Pearls
Left-sided atrial thrombi most commonly originate in the left atrial appendage, which is often poorly visualized on TTE (3,4).
Atrial fibrillation, mitral valve disease, rheumatic heart disease, and hypercoagulable states all increase the risk of left atrial thrombus formation (1,3).
POCUS is a valuable rule-in tool for rapidly identifying intracardiac masses, prompting definitive cardiac imaging and early specialty consultation (5).
In patients with stroke and multiorgan infarction, consider a central embolic source. Early cardiac POCUS may rapidly identify an intracardiac mass and meaningfully alter diagnostic evaluation and management.
AUTHORED BY: RYAN SCHROEDER, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Nguyen T, Vaidya Y. Atrial myxoma. In: StatPearls. StatPearls Publishing; 2025. Updated July 3, 2023. Accessed June 29, 2026. https://www.ncbi.nlm.nih.gov/books/NBK556040/
Scheffel H, Alkadhi H, Plass A, et al. Atrial myxomas and thrombi: comparison of imaging features on CT. AJR Am J Roentgenol. 2009;192(3):639-645.
Donaldson RM, Emanuel RW, Earl CJ. Diagnosis of atrial thrombi by ultrasound. Thorax. 1982;37(7):507-511.
Riley DC, Cordi HP. Emergency department diagnosis of mitral stenosis and left atrial thrombus using bedside ultrasonography. Acad Emerg Med. 2010;17(5):e30-e31.
Ezzeddine FM, Chuang M, Patel K, et al. Point-of-care ultrasound diagnosis of a giant left atrial mass. CASE (Phila). 2022;6(6):243-246.
Solomon SD. Echocardiography Handbook: A Practical Casebook. Humana Press; 2004.
Lee V, Dinh V. Cardiac ultrasound (echocardiography) made easy: step-by-step guide. POCUS 101. Published 2023. Accessed June 29, 2026. https://www.pocus101.com/cardiac-ultrasound-echocardiography-made-easy-step-by-step-guide/