Brain Dead or Baclofen Toxicity?
Overview
Baclofen is a medication used primarily as a muscle relaxant for spasticity; often utilized as an adjunct in treating painful muscle spasms, clonus, and rigidity caused by spinal-cord related diseases such as cerebral palsy, spinal cord injury or multiple sclerosis.
Baclofen overdose/toxicity produces a rapid onset of delirium, respiratory depression, coma, and seizures. In large overdoses the patient can appear brain dead. Supportive care is the mainstay of treatment.
Brain death is defined as the irreversible cessation of cerebral and brainstem functioning and is recognized as equivalent to cardiopulmonary death in the US.
Mechanism
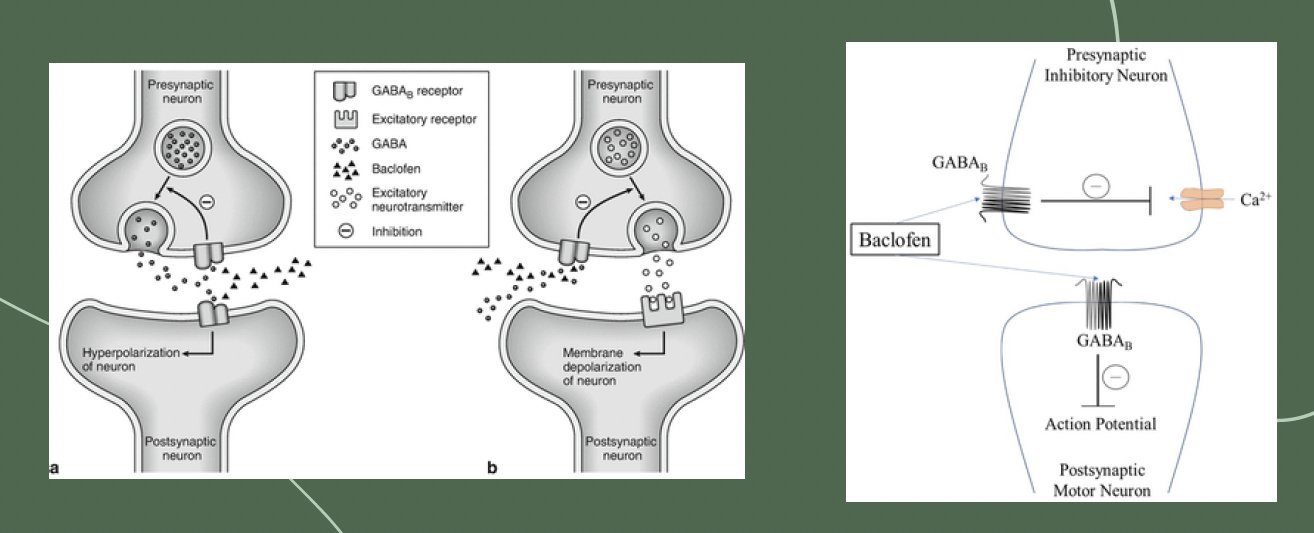
At therapeutic levels it affects mono/polysynaptic reflexes at the spinal level by stimulating GABA-B receptors (GABA is an inhibitory neurotransmitter), inhibiting aspartate and glutamate release contributing to/triggering spasticity and pain (activation of presynaptic GABA-B receptors causes inhibition of excitatory neurotransmitter release within the CNS).
In overdose, selectivity is lost and GABA-B receptors in the brain are targeted, resulting in sedation/coma.
Baclofen also mediates pre- and post-synaptic inhibition (inhibiting the inhibitor) causing seizures in overdose, and like GABA-A withdrawal, the same situation can occur if a patient suddenly stops baclofen and withdrawal symptoms can manifest.
At therapeutic levels it affects mono/polysynaptic reflexes at the spinal level by stimulating GABA-B receptors (GABA is an inhibitory neurotransmitter), inhibiting aspartate and glutamate release contributing to/triggering spasticity and pain (activation of presynaptic GABA-B receptors causes inhibition of excitatory neurotransmitter release within the CNS).
In overdose, selectivity is lost and GABA-B receptors in the brain are targeted, resulting in sedation/coma.
Pharmacokinetics
Rapidly absorbed following oral administration, peak serum levels at ~2 hours
Lipophilic, crosses blood-brain barrier
Relatively small Vd (0.7 L/kg)
Primarily excreted unchanged in urine (65-80% of drug excreted in unchanged form)
15% metabolized by the liver
Mean elimination half-life is 3.5 hours (2-6 hours), can be prolonged in overdose
Half life of intrathecal dosing is ~1-5 hours.
The oral form of baclofen is well absorbed and has a bioavailability of approximately 75%-80% systemically. Fifteen percent is hepatically metabolized and is primarily excreted in the urine with 65%–80% of the drug excreted in its unchanged form. Baclofen’s water solubility does not allow it to readily cross the blood–brain barrier (BBB) when administered orally. Accordingly, oral baclofen may require higher doses to achieve a therapeutic effect and have an increased potential for unwanted side effects, such as somnolence and sedation.
Therapeutic Dosing
Dosing usually starts at ~5 mg po TID, may be gradually escalated as tolerated. Doses available in 5 mg, 10 mg and 20 mg. The package insert recommends a maximal dose of 80 mg/day however in rare cases some patients may be treated with up to ~300 mg/day. It is also available in an intrathecal formulation with doses ranging 50- 1000 mcg/day, this allows for greater concentrations in the spinal cord without higher levels in the brain.
The catheter is placed into the cerebrospinal fluid (CSF) in the subarachnoid space and connected to a pump which is typically inserted into the lower abdominal wall. This pump has a reservoir that can be filled with baclofen. Pump delivers baclofen in small amounts into the CSF causing inhibition at the spinal level.
Toxic Dosing
Acute ingestion >200-400 mg is expected to produce significant CNS toxicity with delirium, coma and paradoxical seizures. However, patients on chronic baclofen therapy may develop tolerance.
One 20 mg tablet can produce a coma in a 10 kg toddler.
Intoxication will develop within 2 hours, delirium is most evident just prior to onset of coma, duration of coma can last 24-48 hours> longer in renal failure
Smaller doses may cause mild drowsiness, lethargy, confusion.
Renal Considerations
Renal dysfunction is a major risk factor for accidental baclofen intoxication. Renal failure increases the half-life of baclofen in an unpredictable fashion, so baclofen should be avoided for GFR <30 ml/min. Even low doses can precipitate encephalopathy in patients with renal dysfunction.
Patients on chronic stable doses of baclofen may still develop toxicity due to an acute kidney injury
In practice, encephalopathy is often due to a combination of factors including baclofen accumulation, uremic encephalopathy and the accumulation of other centrally acting medications (e.g. gabapentin).
Symptoms of Toxicity
In large overdoses, patient can appear brain dead with fixed dilated pupils, hypotonia, and areflexia (including absent brainstem reflexes)
CNS:
Mental status depression (lethargy, confusion, somnolence, hallucinations, agitation, delirium)>> coma
Diminished pupillary response/abnormal pupils> fixed dilated pupils
Loss of brainstem reflexes
Flaccid tone, hyporeflexia with absent DTR
With intrathecal baclofen, ascending hypotonia may occur
Nystagmus, tremor
Paradoxical seizures (generalized tonic/clonic or myoclonic, and/or nonconvulsive status epilepticus)
Cardiovascular:
Sinus bradycardia or tachycardia
Hyper- or hypotension
1st degree heart block and QT prolongation (rare)
Respiratory:
Respiratory depression
Need for intubation and mechanical ventilation
GI:
Nausea/vomiting
Excessive salivation
General: Hypothermia
Differential Diagnosis
Sepsis
Intracranial pathology (trauma, hemorrhage, stroke, mass)
Hypoglycemia
Adrenal crisis
Decompensated hypothyroidism
Opioid intoxication
Toxic ingestions (barbiturates/benzos, carbamazepine, GHB (gammahydroxybutyrate — illicit drug used in nightclubs), toxic alcohols
Management
Basic workup: vitals, (ABCs), ECG, blood glucose, toxicology panel, VBG, CBC, CMP, CK
Discontinue baclofen (caution on withdrawal later in course
For patients on intrathecal baclofen with a pump, consult the managing specialist, interrogate the pump and stop infusion
Can consider activated charcoal for acute ingestion within the first few hours of an acute overdose (50 grams (1 g/kg in children)) in order to reduce the total dose of baclofen absorbed.
It is given with intention of reducing coma and length of ICU stay.
**Use only once the airway has been secured as there is a risk of rapid onset of coma and seizures in overdose with the potential for charcoal pulmonary aspiration/pneumonitis.
Largely supportive> NO antidote:
Reduced GCS and respiratory depression: early intubation and ventilation
Seizures: managed with benzodiazepines
Lorazepam 0.1 mg/kg
Diazepam 0.15 mg/kg
Midazolam 0.2 mg/kg
Hypotension: usually fluid responsive, vasopressors as needed
Management - Dialysis Considerations
In acute overdose, guidelines generally suggest that dialysis should not be performed. However, this is largely based on patients with preserved renal function. Some possible indications for dialysis would include a critically high dose intoxication in a patient with severe renal failure.
In subacute overdose in the context of renal impairment, dialysis is suggested if there is CNS depression/coma requiring mechanical ventilation. Dialysis may also be helpful in patients with marked somnolence/obtundation with a goal of reducing hospital length of stay.
The goal of hemodialysis is to remove enough baclofen for the patient to be extubated and safely protecting their airway (i.e., not obtunded). For patients on chronic baclofen therapy, excessive removal of baclofen could precipitate withdrawal.
Brain Dead or Tox?
The American College of Medical Toxicology (ACMT) notes that baclofen overdose can induce coma that may resemble brain death, with coma lasting up to 5-7 days. It is important to identify any reversible causes of brain injury and to confirm the presence of contributing drugs. At least 5 drug half-lives should be observed to ensure adequate clearance before determining brain death in overdose patients.
Once a patient has recovered from overdose and symptoms of intoxication resolve, it is important to restart the regular baclofen, otherwise a withdrawal state can occur, mimicking ongoing toxicity (occurs 24-48 hr after with seizures, dyskinesia, hallucinations and visual disturbances)
Mean elimination half-life is 3.5 hours (2-6 hours), can be prolonged in overdose>>> can be prolonged in renal dysfunction in unpredictable pattern
Disposition
If a patient is asymptomatic at 4-6 hours, can typically be medically cleared
Minor CNS depression requires medical admission for observation until symptoms resolve
Severe symptoms often require ICU level of care and monitoring
Baclofen Withdrawal
Definition
A dysfunctional condition in which removal of baclofen, an inhibitory neurotransmitter, from the central nervous system (CNS) causes CNS excitation.
It should be noted that patients on chronic oral baclofen can also have withdrawal.
Withdrawal likely results from loss of chronic inhibitory effect on postsynaptic receptors Withdrawal typically occurs 24-48 hours after discontinuation of the drug or a reduction in dose
Causes
Baclofen dose reduction or cessation
Intrathecal pump issues (catheter dislodgement/kinking/ migration)
Reservoir underfilling, pump malfunction
Symptoms
Mimics sx seen with other CNS depressant withdrawal syndromes
Spasticity
Myalgias
Neuropsychiatric
Confusion, altered mental status
Visual hallucinations
Hypertension, tachycardia, hyperthermia
Muscle rigidity
Seizures
Treatment
Supportive
Pump interrogation
AUTHORED BY: KELSIE RHYNE, DO
FACULTY EDITING BY: LAUREN PORTER, DO
References
Dease NM, Kershner EK, Wills BK. Baclofen Toxicity. [Updated 2023 Mar 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK580550/
Farkas, J. (2023, February 12). Baclofen: Therapy, intoxication, & withdrawal. EMCrit Project. https://emcrit.org/ibcc/baclofen/ Ghanavatian S, Derian A. Baclofen. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
Long, N. (2020, November 3). Baclofen toxicity. Life in the Fast Lane • LITFL. https://litfl.com/baclofen-toxicity/
Miller, J. J. (2017). Baclofen overdose mimicking anoxic encephalopathy: A case report and review of the literature. Therapeutic Advances in Drug Safety, 8(5), 165–167.
Neavyn, M. J., Stolbach, A., Greer, D. M., Nelson, L. S., Smith, S. W., Brent, J., & Tormoehlen, L. M. (2017). ACMT position statement: Determining brain death in adults after drug overdose. Journal of Medical Toxicology, 13(3), 271–273.
Romito, J. W., Turner, E. R., Rosener, J. A., Coldiron, L., Udipi, A., Nohrn, L., Tausiani, J., & Romito, B. T. (2021). Baclofen Therapeutics, toxicity, and withdrawal: A narrative review. SAGE Open Medicine, 9, 205031212110221.
Stewart, E., Tormoehlen, L.M. (2016). Baclofen. In: Brent, J., Burkhart, K., Dargan, P., Hatten, B., Megarbane, B., Palmer, R. (eds) Critical Care Toxicology. Springer, Cham.
Swaminathan, A. (2018, March 2). Core em: Intrathecal Baclofen withdrawal. emDOCs.net - Emergency Medicine Education. https://www.emdocs.net/core-em-intrathecalbaclofen-withdrawal/
Wolf E, Kothari NR, Roberts JK, Sparks MA. Baclofen Toxicity in Kidney Disease. Am J Kidney Dis. 2018 Feb;71(2):275-280.