Intern Ultrasound of the Month: Lipomatous Atrial Septal Hypertrophy (LASH) & Other Cardiac Masses
The Case
A 55-year-old female with chronic obstructive pulmonary disease (COPD) presented to the emergency department with one day of worsening shortness of breath that was not responsive to her inhaler or nebulizer at home. She was hypoxic with increased work of breathing and difficulty speaking in full sentences. She had diminished air movement with diffuse expiratory wheezing. Her oxygen saturation improved with supplemental oxygen. As part of the evaluation, point-of-care ultrasound (POCUS) of the heart and lungs was performed to assess cardiac function and evaluate for alternative causes of dyspnea.
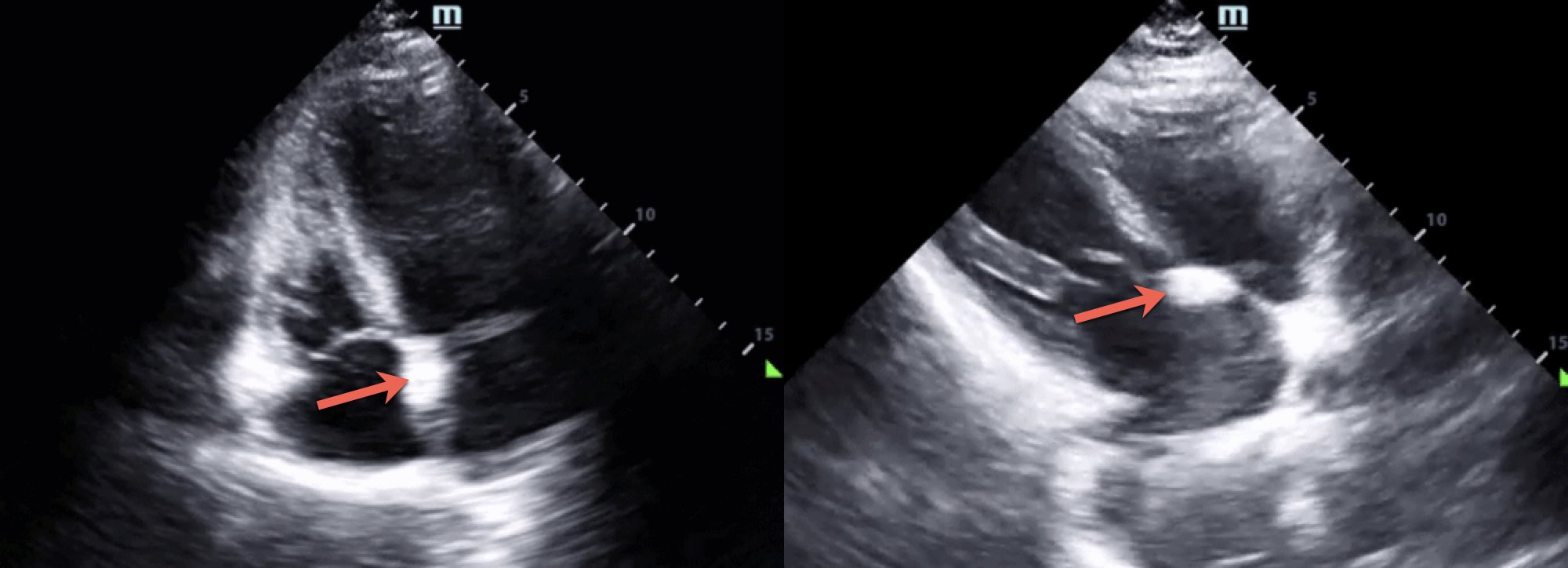
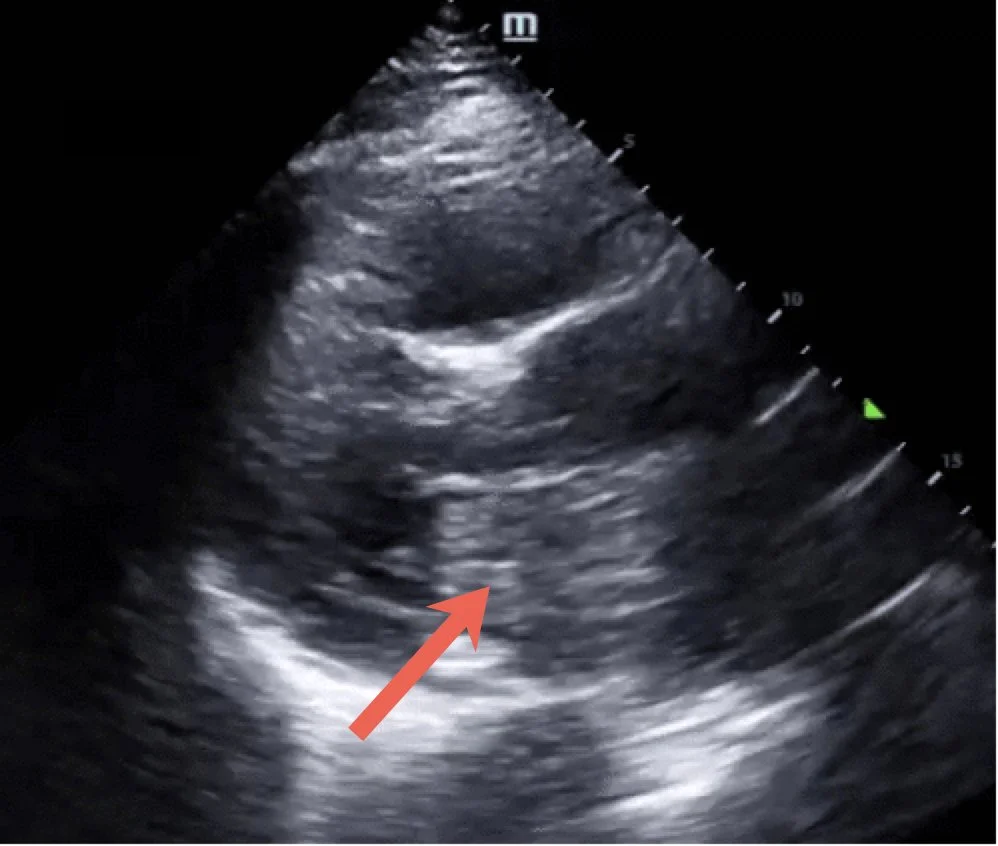
POCUS Findings: Cardiac imaging revealed a hyperechoic mass along the interatrial septum. Review of the patient's prior imaging demonstrated the same finding, which had previously been characterized as lipomatous atrial septal hypertrophy (LASH). The remainder of the cardiac and lung examinations were unremarkable.
Case Conclusion: The patient was treated for a COPD exacerbation with clinical improvement before being discharged home.
Lipomatous Atrial Septal Hypertrophy (LASH)
Lipomatous atrial septal hypertrophy (LASH) is a benign accumulation of adipose tissue within the interatrial septum that can be identified on cardiac ultrasound (1,2). Although typically discovered incidentally, it may be mistaken for other intracardiac masses, including atrial myxoma, thrombus, or infective vegetations (1,3). Recognizing the characteristic appearance of LASH can help avoid unnecessary diagnostic testing while prompting consideration of alternative diagnoses when imaging findings are atypical (3). LASH classically appears as a dumbbell-shaped thickening of the interatrial septum due to sparing of the fossa ovalis, a key imaging feature that helps distinguish it from other cardiac masses (1,2). In contrast, myxomas are typically pedunculated and mobile, often prolapsing through the mitral valve during diastole (4).
Most patients with LASH remain asymptomatic and require no treatment (1,3). However, larger lesions have been associated with cardiac arrhythmias, including supraventricular arrhythmias, such as atrial fibrillation and premature atrial contractions, and atrioventricular block (1). In rare cases, extensive LASH may cause obstructive symptoms such as dyspnea or syncope. Surgical resection is generally reserved for patients with significant symptoms or hemodynamic compromise (1,3).
Other Common Cardiac Masses Confused with LASH
Cardiac myxoma
Myxoma
Cardiac myxomas are benign cardiac tumors most commonly found in the left atrium, typically arising from the atrial septum at the fossa ovalis (unlike LASH). They are often pedunculated and highly mobile, sometimes prolapsing through the mitral valve during diastole. If large enough, they can obstruct intracardiac blood flow and impair cardiac output, often necessitating surgical resection. Myxomas also carry a risk of systemic embolization due to tumor fragmentation or thrombus formation on their surface (4).
Thrombus
Intracardiac thrombus is another important finding that may be identified on cardiac ultrasound. Left atrial thrombi are most commonly seen in patients with atrial fibrillation and typically originate from the left atrial appendage. Recognition of a left atrial thrombus on POCUS has important clinical implications, including assessment of embolic risk and determining whether cardioversion can safely be performed before anticoagulation and confirmatory imaging (5).
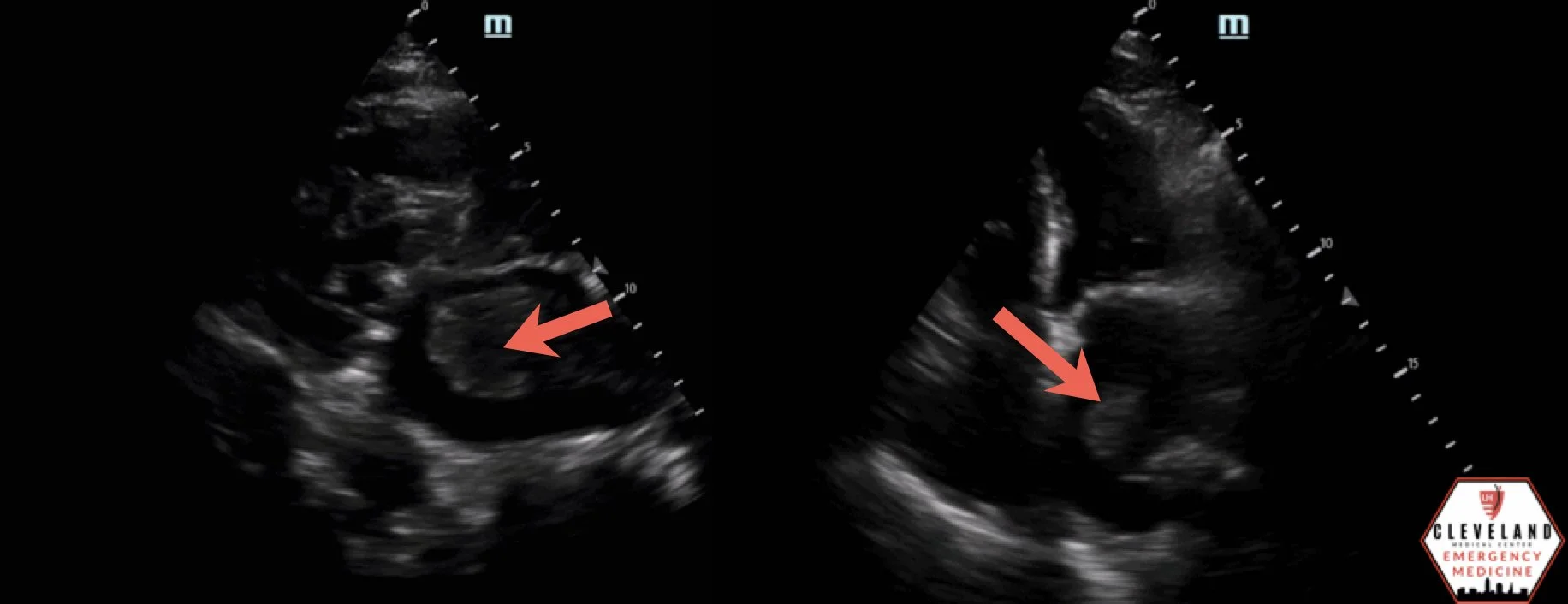

Vegetation on the tricuspid valve
Vegetations
Vegetations are a complication of infective endocarditis and appear as irregular, mobile masses attached to cardiac valves. They develop when bacteria adhere to damaged endocardial surfaces, leading to deposition of fibrin, platelets, and bacterial colonies. Risk factors include prosthetic heart valves, prior infective endocarditis, intravenous drug use, congenital heart disease, and certain valvular abnormalities. Although the diagnosis of infective endocarditis relies on clinical, microbiologic, and imaging findings, the presence of valvular vegetations on echocardiography is a major diagnostic criterion (6).
Take Home Points
LASH is a benign fatty infiltration of the interatrial septum that is often discovered incidentally.
The classic ultrasound appearance is a dumbbell-shaped thickening of the interatrial septum with sparing of the fossa ovalis.
Important POCUS mimics include atrial myxoma, intracardiac thrombus, and infective vegetations.
Consider the lesion's location, attachment, mobility, and clinical context when evaluating intracardiac masses.
When an intracardiac mass cannot be confidently characterized on POCUS, comprehensive echocardiography or advanced cardiac imaging should be obtained.
AUTHORED BY: ASHLEY TIMMRECK-WALKER, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Laura DM, Donnino R, Kim EE, et al. Lipomatous atrial septal hypertrophy: a review of its anatomy, pathophysiology, multimodality imaging, and relevance to percutaneous interventions. J Am Soc Echocardiogr. 2016;29(8):717-723.
Gaillard F, Walizai T, Yap J, et al. Lipomatous hypertrophy of the interatrial septum. Radiopaedia.org. Accessed July 31, 2025.
Nadra I, Dawson D, Schmitz SA, et al. Lipomatous hypertrophy of the interatrial septum: a commonly misdiagnosed mass often leading to unnecessary cardiac surgery. Heart. 2004;90:e66.
Reynen K. Cardiac myxomas. N Engl J Med. 1995;333(24):1610-1617.
Datta A, Kapoor M, Pearl-Davis M, et al. Emergency ultrasound diagnosis of a left atrial thrombus and diffuse emboli. Crit Ultrasound J. 2011;3:93-95.
Cabell CH, Abrutyn E, Karchmer AW. Bacterial endocarditis. Circulation. 2003;107(20).