Intern Ultrasound of the Month: Achilles Tendon Rupture
The Case
A 40-year-old male presented to the emergency department with sudden onset, severe posterior right ankle pain that occurred while playing basketball. After this, he was unable to ambulate normally but could bear weight with difficulty. He noted a recent calf strain in that leg but no other prior injuries.
On exam, the patient appeared uncomfortable due to pain. His right calf appeared larger than his left and was diffusely tender to palpation. He was unable to actively plantarflex his right foot, and squeezing the calf did not produce any passive plantarflexion, i.e. a positive Thompson test. Sensation and perfusion were intact, and he had no tenderness over his malleoli, foot, or more proximal leg.
Because he was able to bear weight and had no focal bony tenderness, radiographs were deferred due to low suspicion for fracture. Given the high clinical suspicion for Achilles tendon rupture, point-of-care ultrasound (POCUS) was performed.
Long axis view of the Achilles tendon

Short axis view of the Achilles tendon
POCUS findings: Ultrasound demonstrated disruption of the normal fibrillar architecture of the distal Achilles tendon with tendon discontinuity and an associated hypoechoic fluid collection, consistent with a complete Achilles tendon rupture.
Case Conclusion: The patient was placed in a splint in plantarflexion. Orthopedic surgery was called to help facilitate follow up and elected to see the patient in the ED, which ultimately helped expedite surgical intervention.
—-
Achilles Tendon Tear
Epidemiology
Achilles tendon ruptures are common and have increased in incidence over time. A Swedish nationwide registry study from 2001 to 2012 found that men had an incidence of Achilles tendon rupture of 47 per 100,000 person-years at the beginning of the study period, increasing to 55.2 by the final year. In women, incidence rose from 12.0 the first year to 14.7 per 100,000 person-years over the same period, suggesting a gradual rise in overall incidence (1). A population-based study from Ontario, Canada from 2003 to 2013 demonstrated a similar trend, with incidence increasing from 18.0 to 29.3 per 100,000. Men aged 40-49 had the highest incidence of injury (2). Collectively, these studies demonstrate that Achilles tendon rupture most commonly affects middle-aged men and frequently occurs during recreational athletic activity. (1,2).
POCUS Assessment
POCUS is performed using a high-frequency linear probe with the patient positioned supine or prone and the foot allowed to hang off the edge of the bed to keep the Achilles tendon relaxed. Evaluate the tendon in both long-axis and short-axis views, starting distally at the calcaneal insertion and tracking proximally along its course (3). The long-axis view best demonstrates the normal fibrillar architecture of the tendon, while the short-axis view helps assess tendon thickness and surrounding soft tissues.
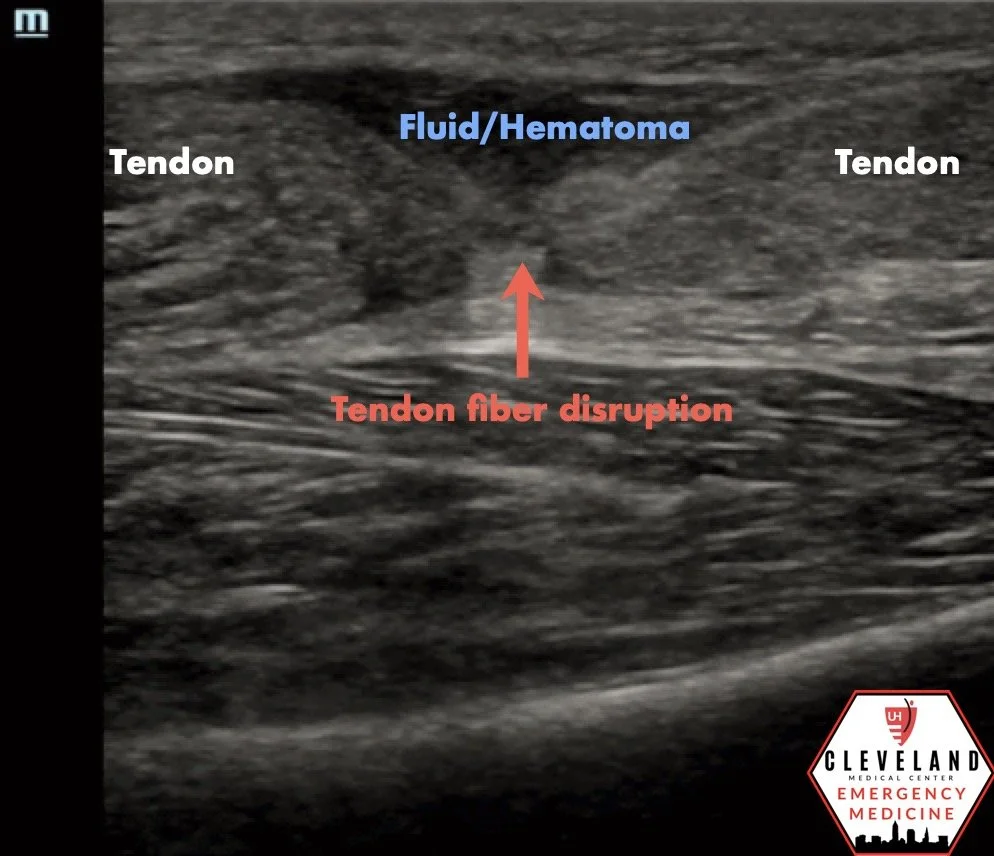
On a normal exam, the Achilles tendon appears as a tightly organized, linear, fibrillar structure. In the setting of rupture, ultrasound demonstrates loss of normal fibrillar architecture with discontinuity of tendon fibers. A hypoechoic gap representing hematoma or fluid may be seen between retracted tendon ends (3-5).
Dynamic assessment is a key component of the ultrasound evaluation. Passive dorsiflexion of the foot while maintaining the probe over the area of abnormality allows assessment of tendon continuity. Widening of a hypoechoic defect with dorsiflexion is highly suggestive of a complete rupture, whereas preserved continuity with movement suggests a partial tear (4-5).
Ultrasound can also identify associated hematoma and evaluate for alternative diagnoses when the clinical presentation is less straightforward (4). Overall, POCUS provides a rapid bedside assessment that supports the diagnosis, differentiates complete from partial tears, and facilitates timely orthopedic consultation (3–5).
Pearls & Pitfalls
A common early pitfall is failure to adequately visualize the Achilles tendon due to the probe slipping off the narrow, curved anatomy of the posterior ankle. Careful probe stabilization, consistent contact with the skin, and maintaining the tendon within the imaging plane are essential throughout the examination.
Dynamic assessment augments the exam and improves diagnostic confidence. Passive dorsiflexion of the foot while maintaining the probe over the area of concern allows evaluation of tendon continuity. Widening of a hypoechoic defect with movement supports a full thickness rupture (4). Conversely, partial thickness tears more commonly involve the superficial fibers (the area bearing the greatest amount of force in most patients) and appear as focal loss of tendon linearity and organization without complete discontinuity (5).
Anisotropy is a common ultrasound artifact when evaluating tendons. If the ultrasound beam is not perpendicular to the tendon, the normal fibrillar architecture may appear artificially hypoechoic, potentially mimicking tendinopathy or a partial tear. Small adjustments of the probe help maintain a perpendicular beam and minimize this artifact.
When findings are subtle, comparison with the contralateral Achilles tendon can improve diagnostic confidence by highlighting differences in tendon thickness, echotexture, and fiber continuity.
Ultrasound can also help differentiate Achilles tendon rupture from mimics such as abscess. When applying probe compression over the affected area, echogenic swirling debris suggests purulence. However, reactive or hemorrhagic fluid associated with acute tendon rupture may also demonstrate movement with compression, making clinical context and accompanying sonographic findings essential for accurate interpretation (4).
Clinical Significance
Complete Achilles tendon rupture can result in significant functional impairment, particularly in patients with high physical demands, including athletes, younger individuals, and manual laborers. Accurate diagnosis is essential to guide management, facilitate appropriate follow-up, and provide useful information to consulting surgeons when determining whether operative intervention may be beneficial (6).
A 2019 systematic review and meta-analysis including 29 studies (10 randomized controlled trials) demonstrated a lower risk of re-rupture with operative management compared to non-operative treatment (2.3% vs 3.9%, p<0.001). Operative management, however, was associated with a higher overall complication rate (4.9% vs 1.6%, p<0.001), largely due to infections. Notably, when accelerated functional rehabilitation with early range of motion was employed, differences in re-rupture rates between operative and non-operative management were no longer observed (6). As a result, operative management is not required for all patients and should be individualized, with risks and benefits discussed in consultation with orthopedic surgery.
Management
Pain control is an important component of initial management, as patients are often significantly uncomfortable. Definitive treatment should be guided by orthopedic consultation and may include operative repair or conservative management. For patients not proceeding directly to surgery, immobilization with the ankle placed in approximately 20 degrees of plantarflexion is recommended. Evidence guiding management of partial Achilles tendon tears is more limited. However, these injuries generally respond well to non-operative management (7).
Clinical Pearls
Physical examination remains essential when evaluating suspected Achilles tendon rupture.
A positive Thompson test (absence of passive plantarflexion with calf squeeze) is highly suggestive of a complete rupture (8).
Partial tears may preserve plantarflexion and are often more readily identified with POCUS (5).
Take-Home Points
Maintain a high index of suspicion for Achilles tendon rupture in patients with a sudden "pop" or lower leg pain, especially after activity.
A positive Thompson test is highly suggestive of a complete rupture, but preserved plantarflexion does not exclude a partial tear.
POCUS rapidly confirms the diagnosis, differentiates complete from partial tears, and expedites orthopedic consultation.
Dynamic assessment with passive dorsiflexion improves evaluation of tendon continuity and increases diagnostic confidence.
AUTHORED BY: CALVIN JACKSON, MD
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Huttunen TT, Kannus P, Rolf C, Felländer-Tsai L, Mattila VM. Acute Achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. Am J Sports Med. 2014;42(10):2419–2423.
Sheth U, Wasserstein D, Jenkinson R, Moineddin R, Kreder H, Jaglal SB. The epidemiology and trends in management of acute Achilles tendon ruptures in Ontario, Canada: a population-based study of 27 607 patients. Bone Joint J. 2017;99-B(1):78–86.
Hryniw C. Achilles tendon rupture. Core Ultrasound. January 25, 2023. Accessed July 13, 2025. https://coreultrasound.com/achilles-tendon/
Noble VE, Nelson BP. Manual of emergency and critical care ultrasound. 2nd ed. Cambridge University Press; 2011.
Alfredson H, Masci L, Öhberg L. Partial mid-portion Achilles tendon ruptures: new sonographic findings helpful for diagnosis. Br J Sports Med. 2011;45(5):429–432. doi:10.1136/bjsm.2009.067298
Ochen Y, Beks RB, van Heijl M, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364:k5120. doi:10.1136/bmj.k5120
American Academy of Orthopaedic Surgeons. Achilles tendon rupture (tear). OrthoInfo. Accessed July 13, 2025. https://www.orthoinfo.org/en/diseases--conditions/achilles-tendon-rupture-tear/
Thompson TC. A test for rupture of the tendo Achillis. Acta Orthop Scand. 1962;32:461–465.