Mixed (acid/base) Feelings on Salicylates
What are Salicylates?
Salicylates is the broad term used for Acetylsalicylic acid (ASA), salicylic acid, and their derivatives
Acetylsalicylic acid (ASA) is the active ingredient of aspirin
Irreversible cyclooxygenase-1 inhibitor that is used as an analgesic, antipyretic, anti-inflammatory, and antiplatelet drug
ASA is a common medication used by many ED patients for the management of cardiovascular events (e.g., acute MI, angina) and for primary/secondary prophylaxis of cardiovascular disease
History
The earliest evidence of salicylate use comes from Sumerian clay tablets, where willow bark was noted for its pain-relieving properties
In 1828, a German chemist named Johann Andreas Buchner isolated a yellow substance from willow bark and named it salicin, after the Latin name for white willow (Salix alba)
By the late 1800s, large-scale production of salicylic acid began for pain and fever treatment
Bayer marketed it under the brand name Aspirin in 1899, revolutionizing pain management
Pathophysiology of Toxicity
Directly stimulate the respiratory center of the brain causing hyperventilation and CO2 washout leading to a primary respiratory alkalosis
Mitochondrial toxin that uncouple the electrons from ATPase in the electron chain transport resulting in cessation of oxidative phosphorylation
Organic products such as lactate, keto acids and pyruvate that are generated as a result of uncoupling of the electron chain transport drive a metabolic acidosis
As a result, you have a “mixed picture” acid-base disturbance with a primary respiratory alkalosis followed by metabolic acidosis
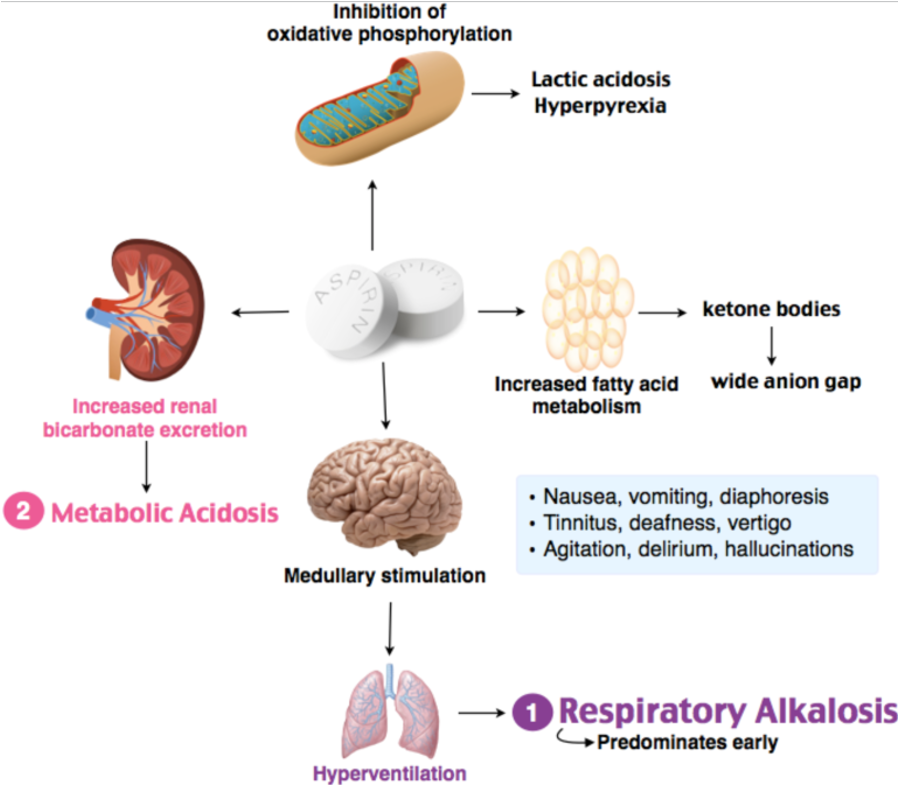
Figure 1. Pathophysiology of salicylate toxicity. Adapted from Salicylate toxicity, Rosh Review
Clinical Features
Early symptoms: tinnitus, nausea, vomiting, tachypnea, hyperpnea
Late symptoms: hyperthermia, agitation, delirium, seizures, noncardiogenic pulmonary edema
Also known to be an imitator of sepsis (hyperthermia, hypotensive, lactate, altered, respiratory distress)
Common offenders: Aspirin (often intentional overdose), bismuth subsalicylate, oil of wintergreen (methyl salicylate), and excessive use of pain relief creams i.e. Aspercreme, BenGay.
Perspective: 1 tablespoon of oil of wintergreen = equivalent of 7g of aspirin
Labs/Workup
Initial labs should include VBG, salicylate level and CMP
Therapeutic salicylate range = 10-15 mg/dL
Toxicity is a concern with ingestion of 150 mg/kg or more
Toxicity in adults starts around 30 mg/dl and at 20 mg/dl in kids
Because salicylate levels may be falsely low within 4 hours of ingestion and do not necessarily correlate with clinical presentation, a high index of suspicion should be maintained when caring for a patient with symptoms of salicylate poisoning
Treatment
Alkalinize then Dialyze
The definitive treatment is dialysis
Treatment should be based on the clinical picture, but if approaching 90 mg/dL (inn acute toxicity), then it may be worth empirically dialyzing
Until dialysis can be initiated, the goal is to treat the acidosis
At a physiologic serum pH, salicylic acid exists in an ionized state as a weak acid; in toxicity (acidic environment), it is converted to an un-ionized (highly permeable) state
First step is to initiate IV sodium bicarbonate bolus (1-2 mEq/kg) and infusion (150 mEq (3 amps) in 1 L of 5% dextrose in water (D5W) at 1.5-2 times maintenance)
Goal serum pH = 7.45-7.55
Bicarbonate infusion creates a higher pH which Ion traps salicylates in the urine
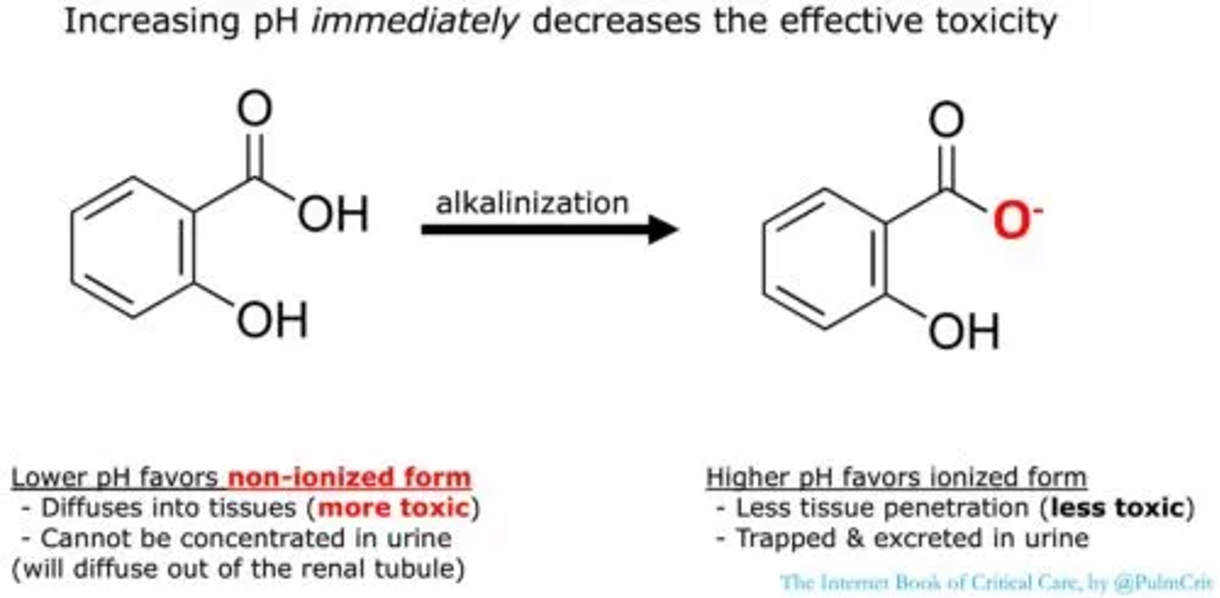
Figure 2. Ionization of salicylic acid with alkalinization. Adapted from Salicylate intoxication, EMCrit Project
As with most metabolic acidosis, you want to avoid intubation as much as possible as patients are able to compensate more effectively from a respiratory standpoint than the ventilator.
If necessary, these patients make good candidates for awake/delayed intubation.
Will require larger tidal volumes and respiratory rate to compensate for metabolic acidosis
Ongoing care
Patients requiring frequent blood gasses, sodium bicarbonate infusions, or emergent dialysis will require ICU level care
Consider psychiatric consultation for acutely suicidal patients
Discharge may be considered after 6 hours if the patient has down trending levels less than 30, is asymptomatic and maintains a normal pH.
AUTHORED BY: JAKE PERINO, MD, PGY3
FACULTY EDITING BY: LAUREN PORTER, DO
References
American College of Medical Toxicology. Guidance document: management priorities in salicylate toxicity. J Med Toxicol. 2015;11(1):149-152.
Katz K, Koons A. Salicylate poisoning. In: Johnson W, Nordt S, Mattu A, Swadron S, eds. CorePendium. Burbank, CA: CorePendium LLC; updated May 5, 2021. Accessed March 14, 2024. https://www.emrap.org/corependium/chapter/recdUAKgBNpqpYseX/Salicylate-Poisoning
Dargan PI. An evidence-based flowchart to guide the management of acute salicylate (aspirin) overdose. Emerg Med J. 2002;19(3):206-209.
Ciejka M, Nguyen K, Bluth MH, Dubey E. Drug toxicities of common analgesic medications in the emergency department. Clin Lab Med. 2016;36(4):761-776.
Gummin DD, Mowry JB, Spyker DA, et al. 2018 annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 36th annual report. Clin Toxicol (Phila). 2019;57(12):1220-1413.
ResearchGate. Chemical structures of salicylic acid and its synthetic and natural derivatives. Accessed March 14, 2024. https://www.researchgate.net/figure/Chemical-structures-of-salicylic-acid-and-its-synthetic-and-natural-derivatives_fig1_284693818
Farkas J. Salicylate intoxication. EMCrit Project. Published February 12, 2023. Accessed March 14, 2024. https://emcrit.org/ibcc/salicylates/
Salicylate toxicity. Rosh Review. Published February 8, 2023. Accessed March 14, 2024. https://www.roshreview.com/