Intern Ultrasound of the Month: Rotator Cuff Injury
The Case
A 60-year-old male presented to the emergency department for acute right shoulder pain and right upper extremity weakness after doing some mechanical work. While using a tool, he felt a sudden pulling sensation in his shoulder with pain radiating into the neck and upper back.
Physical examination was notable for tenderness over the lateral shoulder, bicipital groove, and posterior shoulder. Active range of motion was limited by pain, with inability to abduct the arm beyond 90°. Passive range of motion also elicited pain. Sensation and distal neurovascular examinations were intact. X-rays of the shoulder demonstrated no acute fracture or dislocation but showed moderate acromioclavicular and glenohumeral osteoarthritis. A musculoskeletal point-of-care ultrasound (POCUS) was performed to better evaluate for rotator cuff tears.
POCUS Findings: There was discontinuity and heterogeneity of the proximal biceps tendon and supraspinatus tendon, concerning for tendon tears. A complex echogenic glenohumeral joint effusion was also present. No sonographic evidence of shoulder dislocation was identified.
Transverse (short-axis) view of the long head of the biceps tendon demonstrating tendon heterogenity with surrounding fluid.
Longitudinal (long-axis) view of the long head of the biceps tendon demonstrating tendon heterogeneity, discontinuity, and surrounding hypoechoic fluid, consistent with tendon tear.
Another longitudinal (long-axis) view of the long head of the biceps tendon demonstrating the transition from abnormal proximal tendon (far left) to preserved distal fibrillar architecture (screen right)
Long-axis view of the supraspinatus tendon demonstrating tendon heterogeneity and discontinuity consistent with a full-thickness rotator cuff tear.
Another long-axis view of the supraspinatus tendon
View of the posterior shoulder demonstrating an echogenic effusion overlying the glenohumeral joint
Case Conclusion: Given his persistent pain, along with POCUS findings, the patient was admitted for pain control. MRI demonstrated full-thickness tears of the supraspinatus and long head of the biceps tendon, in addition to a large glenohumeral joint effusion.
Orthopedic surgery was consulted. Although no acute surgical intervention was indicated, close outpatient follow-up was arranged.
Shoulder Injuries
Background
Shoulder pain is a common emergency department (ED) complaint and one of the most common musculoskeletal presentations in the ED, accounting for up to 8% of ED visits (1). The shoulder is a complex musculoskeletal joint, and understanding its anatomy is essential for accurate ultrasound evaluation.
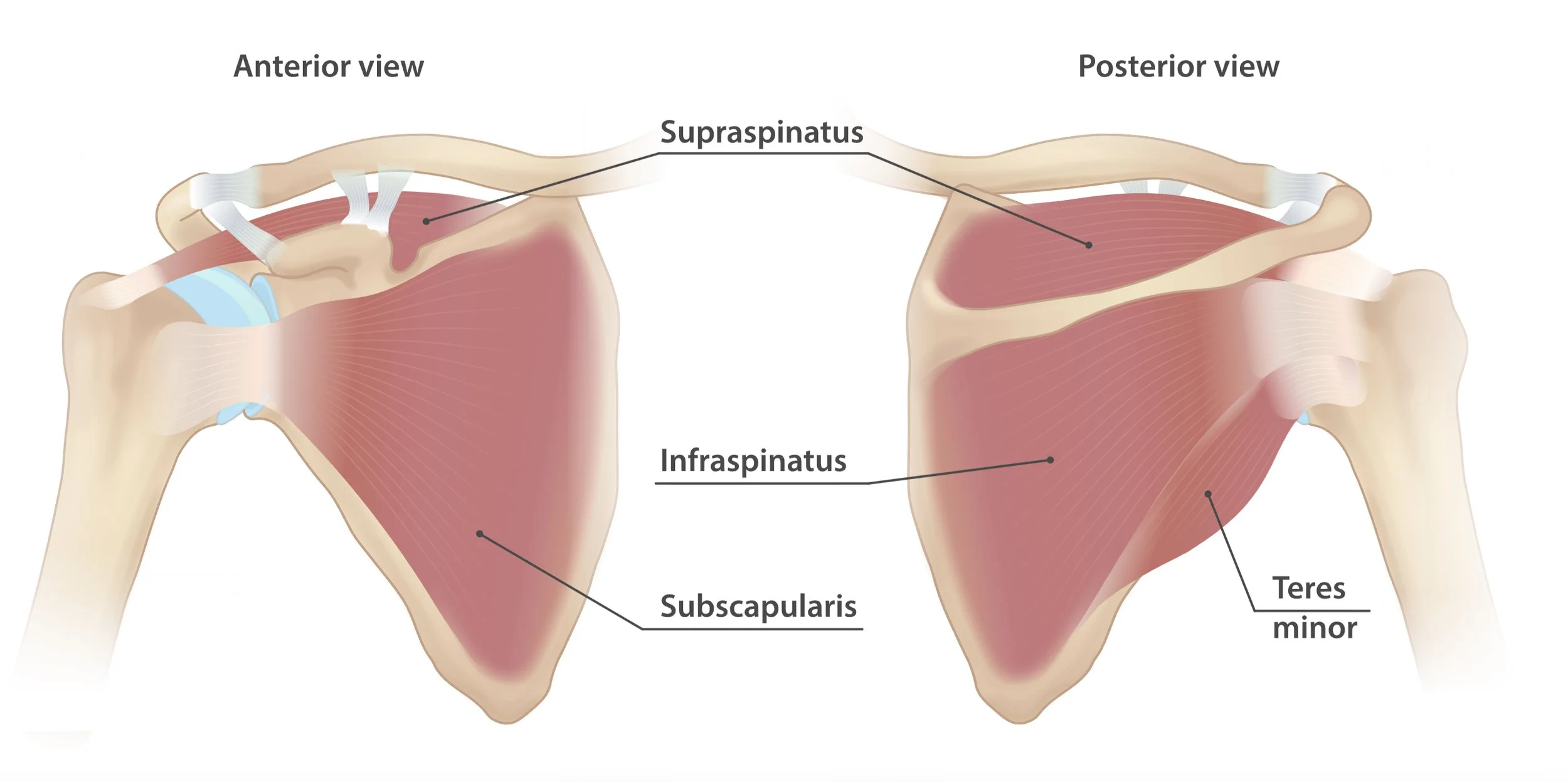
Figure 1. Anatomy of the rotator cuff muscles (anterior and posterior views).
Reproduced from InjuryMap via Wikimedia Commons under the CC BY-NC-SA license. https://commons.wikimedia.org/wiki/File:Rotator_cuff_muscles.svg
The glenohumeral joint is a synovial ball-and-socket joint stabilized by the rotator cuff muscles, tendons, labrum, ligaments, and joint capsule. The rotator cuff consists of the supraspinatus, infraspinatus, subscapularis, and teres minor muscles, which originate from the scapula and insert on the greater and lesser tuberosities of the humerus. The subscapularis inserts on the lesser tuberosity, whereas the supraspinatus, infraspinatus, and teres minor insert on the greater tuberosity. The long head of the biceps tendon originates from the supraglenoid tubercle and superior labrum before coursing through the bicipital groove (2,3). Together, these structures provide dynamic stabilization of the glenohumeral joint while facilitating shoulder motion. The supraspinatus initiates shoulder abduction, the infraspinatus provides external rotation, the subscapularis provides internal rotation, and the long head of the biceps contributes additional glenohumeral stability (3).
Rotator cuff tears commonly result from chronic degenerative changes, repetitive microtrauma, or acute trauma. Degenerative tears become increasingly prevalent with age, whereas acute tears are more commonly associated with forceful traction or shoulder trauma (4). Although many rotator cuff injuries are initially managed conservatively, prompt diagnosis facilitates timely orthopedic evaluation, particularly for patients with acute full-thickness tears (5).
Patients with rotator cuff injuries typically present with shoulder pain, weakness, and limited range of motion following either acute trauma or chronic overuse. Full-thickness tears often produce significant weakness, particularly with shoulder abduction or external rotation, whereas partial-thickness tears may present primarily with pain despite preserved strength. Although physical examination maneuvers can increase suspicion for rotator cuff injury, ultrasound provides direct visualization of the tendon and can help distinguish tendon tears from other causes of shoulder pain (4).
Point-of-care ultrasound (POCUS) provides a rapid, dynamic bedside evaluation of the rotator cuff and long head of the biceps tendon. In experienced hands, ultrasound demonstrates excellent diagnostic accuracy for rotator cuff pathology, with reported sensitivities of approximately 92% and specificities of 94% for full-thickness tears (6). In addition to identifying tendon tears, POCUS can detect associated findings such as biceps tendon pathology, glenohumeral joint effusions, and shoulder dislocation, facilitating timely diagnosis and appropriate orthopedic referral (7,8).
Image Acquisition
A high-frequency linear transducer is the preferred probe for shoulder ultrasound. The examiner may stand either facing the patient or behind the patient while scanning. A systematic examination includes evaluation of the long head of the biceps tendon, subscapularis, supraspinatus, infraspinatus, and acromioclavicular joint. Ideally, each structure should be evaluated dynamically in both the transverse and longitudinal planes. Maintaining the transducer perpendicular to the tendon minimizes anisotropy, an artifact that can mimic tendon pathology by making a normal tendon appear hypoechoic (7,8).
Long Head of the Biceps Tendon
Evaluation of the long head of the biceps tendon begins with the transducer placed transversely over the intertubercular (bicipital) groove on the anterolateral aspect of the humerus. The tendon is first identified in the transverse (short-axis) plane. The transducer is then rotated 90° to obtain the longitudinal (long-axis) view (7,8).

Figure 2. Probe placement for evaluating long head of biceps in transverse view (left) and longitudinal view (right)
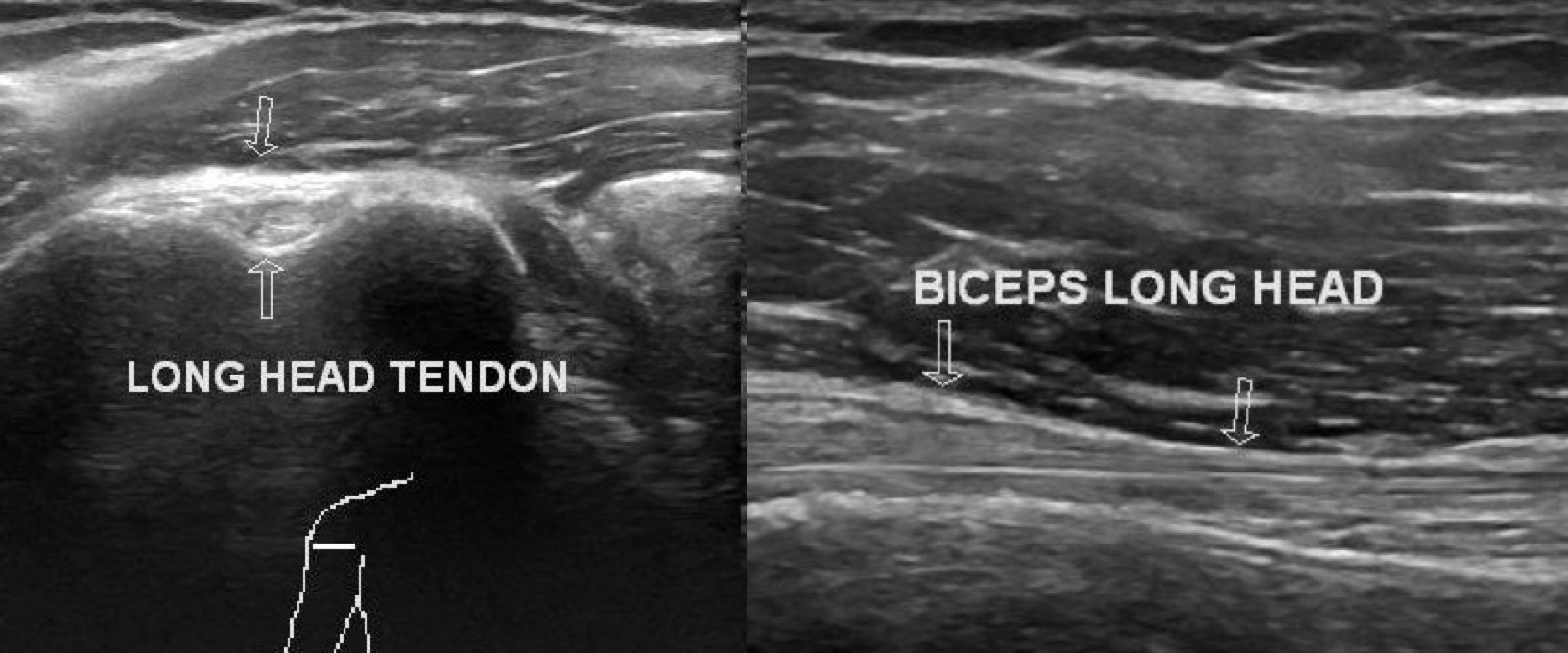
Figure 3. Long head of the biceps tendon tear.
Adapted from Patel MS. Biceps long head tendon tear. Radiopaedia.org. under the CC BY-NC-SA license.
Subscapularis Tendon
The subscapularis tendon is evaluated with the patient's arm externally rotated to expose its insertion on the lesser tuberosity. The transducer is placed over the anterior shoulder using the lesser tuberosity as a key sonographic landmark. Once the longitudinal view has been obtained, the transducer is rotated 90° to obtain the transverse view (7,8).
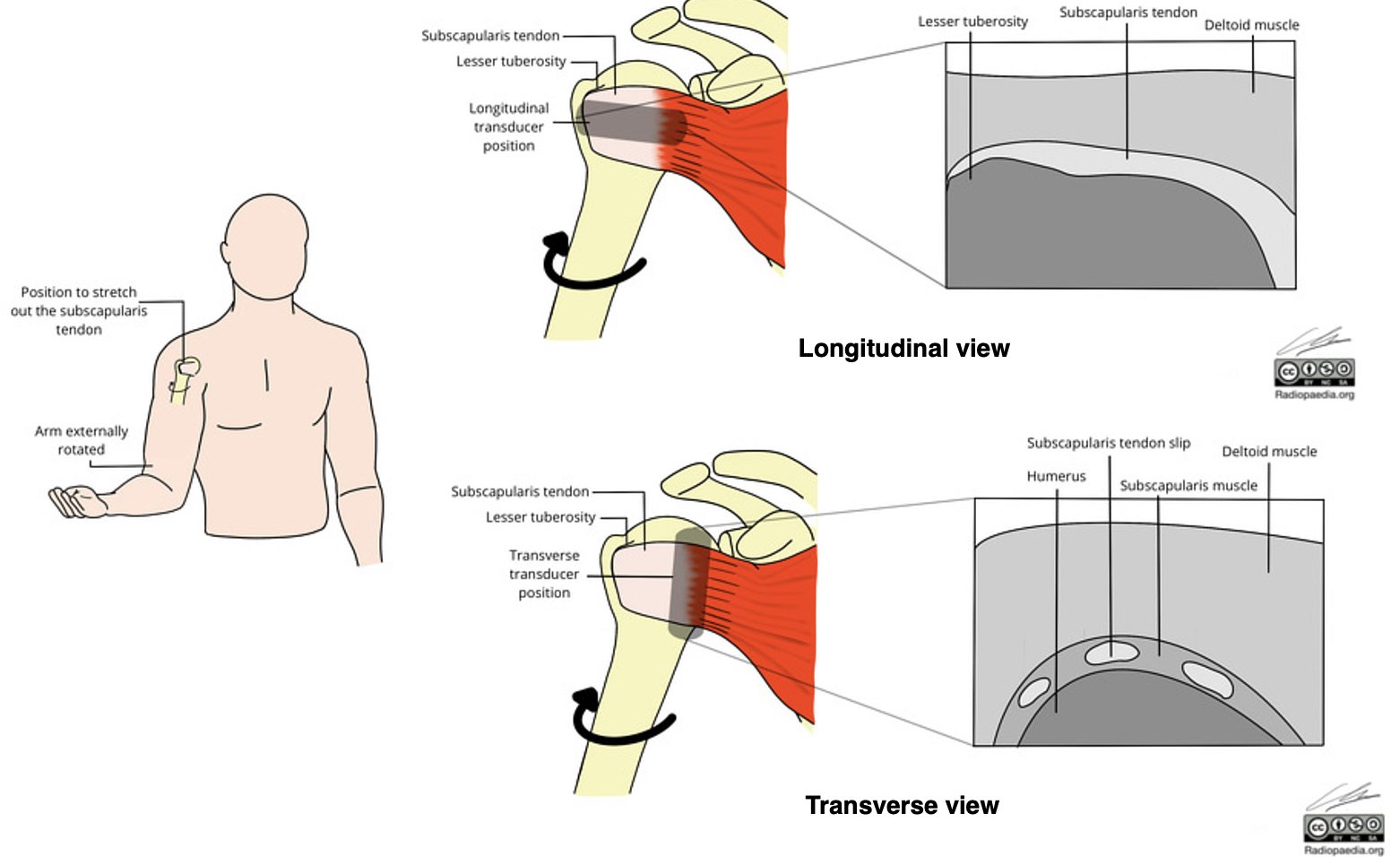
Figure 4. Probe placement for obtaining a longitudinal and transverse views of the subscapularis tendon with the shoulder externally rotated.
Adapted from Patel M. Shoulder ultrasound: subscapularis identification (illustration).Radiopaedia.org. under the CC BY-NC-SA license.
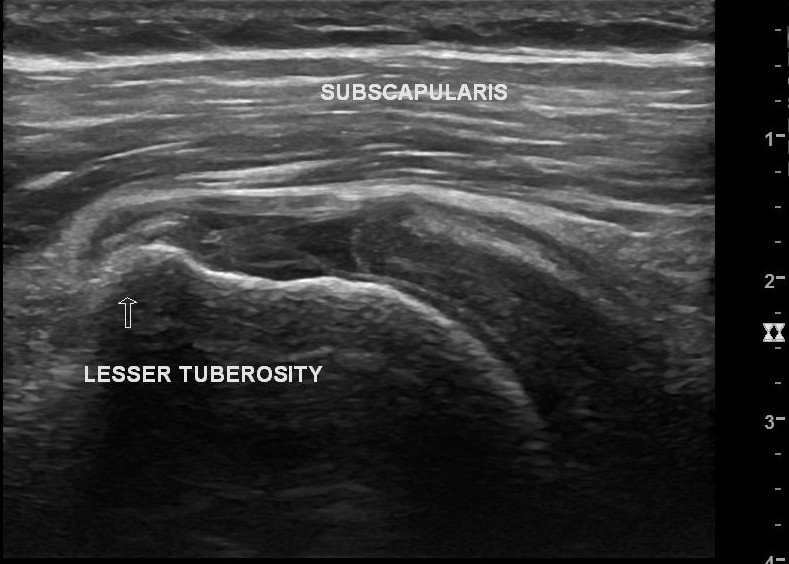
Figure 5. Subscapularis tear.
Reproduced from Patel M. Subscapularis tendon tear (preoperative and postoperative ultrasound). Radiopaedia.org. under the CC BY-NC-SA license.
Supraspinatus Tendon
The supraspinatus tendon is best evaluated with the patient's elbow flexed and the hand placed behind the back in the modified Crass position (Figure 6). This position rotates the greater tuberosity anteriorly and away from the acromion, optimizing visualization of the supraspinatus tendon within the subacromial space. The transducer is positioned over the anterolateral shoulder, centered on the greater tuberosity, to obtain longitudinal and transverse views of the supraspinatus tendon (7,8).

FIgure 6. Probe placement for evaluating the longitudinal view of the supraspinatus.
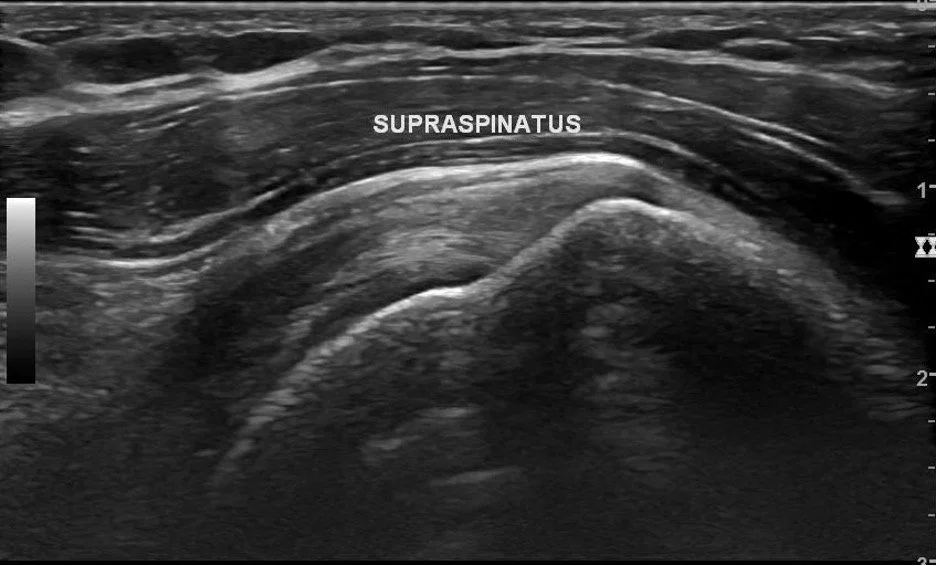
Figure 7. Supraspinatus tendon.
Adapted from Patel MS. Long head of biceps tendon tear. Radiopaedia.org. under the CC BY-NC-SA license.
Figure 8. Our patient’s supraspinatus tear for comparison.
Infraspinatus Tendon
The infraspinatus tendon is evaluated from the posterior shoulder. The transducer is placed just inferior to the scapular spine and moved laterally until the posterior aspect of the humeral head is visualized. Longitudinal and transverse views are obtained by rotating the transducer 90° (7,8).

FIgure 10. Probe placement for evaluating the longitudinal view of the infraspinatus.
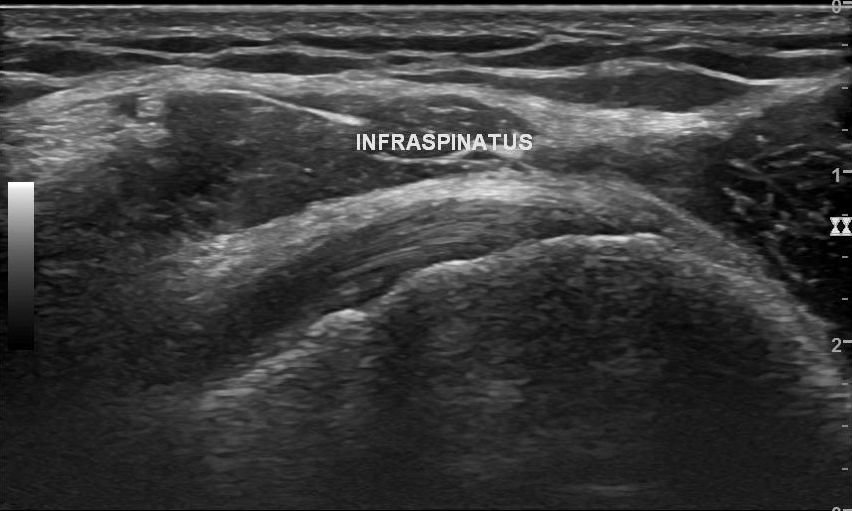
Figure 10. Infraspinatus tendon.
Reproduced from Patel MS. Long head of biceps tendon tear. Radiopaedia.org. under the CC BY-NC-SA license.
Ultrasound Findings
Full-thickness tear: Complete tendon discontinuity with a hypoechoic or anechoic fluid-filled defect.
Partial-thickness tear: Focal hypoechoic or mixed echogenic defect within the tendon (7-9).
Biceps tendon injury: Tendon discontinuity, medial subluxation or dislocation, or surrounding peritendinous fluid.
Joint effusion: Anechoic or complex fluid within the glenohumeral joint (7,8).
Take-Home Points
Evaluate each rotator cuff tendon in both the transverse and longitudinal planes.
Optimize tendon visualization with proper patient positioning and probe placement.
Full-thickness rotator cuff tears demonstrate complete tendon discontinuity with a hypoechoic or anechoic fluid-filled defect.
POCUS is an accurate bedside tool for evaluating rotator cuff tears, biceps tendon injuries, and associated shoulder pathology.
AUTHORED BY: AUBREY COVINGTON, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Fontánez R, Ramos-Guasp W, Ramírez H, De Jesús K, Conde JG, González J, Frontera WR. Musculoskeletal conditions in the emergency room: a teaching opportunity for medical students and residents. P R Health Sci J. 2021;40(2):68-74.
Kadi R, Milants A, Shahabpour M. Shoulder anatomy and normal variants. J Belg Soc Radiol. 2017;101(Suppl 2):3.
Miniato MA, Anand P, Varacallo MA. Anatomy, shoulder and upper limb, shoulder. In: StatPearls. StatPearls Publishing; updated July 24, 2023. Accessed July 8, 2026.
Bonz JW, Tinloy B. Emergency department evaluation and treatment of the shoulder and humerus. Emerg Med Clin North Am. 2015;33(2):297-310.
Sørensen AKB, Bak K, Krarup AL, et al. Acute rotator cuff tear: do we miss the early diagnosis? A prospective study showing a high incidence of rotator cuff tears after shoulder trauma. J Shoulder Elbow Surg. 2007;16(2):174-180.
Smith TO, Back T, Toms AP, Hing CB. Diagnostic accuracy of ultrasound for rotator cuff tears in adults: a systematic review and meta-analysis. Clin Radiol. 2011;66(11):1036-1048.
Jacobson JA. Shoulder US: anatomy, technique, and scanning pitfalls. Radiology. 2011;260(1):6-16.
Singh JP. Shoulder ultrasound: what you need to know. Indian J Radiol Imaging. 2012;22(4):284-292.
Yoon YC. Ultrasonography of the rotator cuff. J Korean Soc Ultrasound Med. 2006;25:109-125.