Intern Ultrasound of the Month: Placental Abruption

Representative transabdominal ultrasound demonstrating a retroplacental hematoma consistent with placental abruption. Reproduced from Ali MI. Placental abruption. Radiopaedia.org under the CC BY-NC-SA 4.0 license (6).
The Case
A young female presented to the emergency department as a trauma activation after she was involved in a high-speed motor vehicle collision and was intubated in the field for airway protection. On arrival, she was noted to have a gravid abdomen and spontaneous vaginal bleeding, prompting immediate obstetrics (OB) consultation and transabdominal point-of-care ultrasound (POCUS).
POCUS findings: A live intrauterine pregnancy at approximately 20 weeks gestation with isoechoic area retroplacental collection, raising concern for retroplacental hematoma — see representative image (right). Color Doppler demonstrated no internal blood flow within the collection, further supporting diagnosis. In the setting of blunt abdominal trauma, these findings were highly concerning for placental abruption.
Case Conclusion: The patient was stabilized in the intensive care unit. Despite supportive management, subsequent imaging remained concerning for placental abruption, fetal heart tones were lost shortly after, and the patient underwent dilation and evacuation.
Placental Hematoma/Abruption
Placental abruption is defined as the premature separation of the placenta from the uterine wall prior to fetal delivery and occurs in approximately 0.6–1.2% of pregnancies (1). Various factors can contribute to placental abruption, including trauma, as in our case. Shearing forces caused by blunt abdominal trauma result in bleeding along the decidual-placental interface, allowing blood to accumulate in the preplacental, intraplacental, or retroplacental space (1).
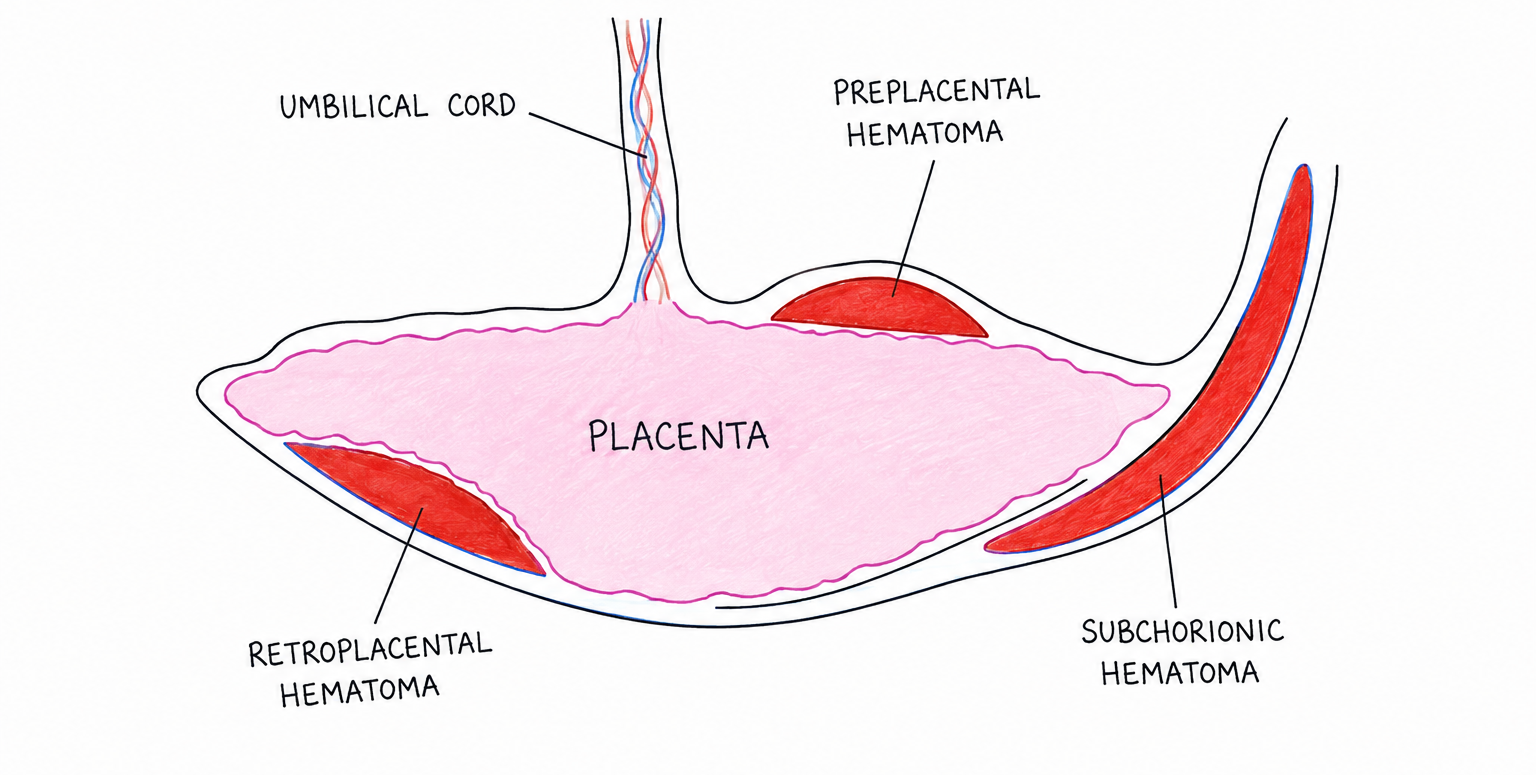
Schematic illustrating the potential locations of placental hemorrhage, including preplacental, retroplacental, and subchorionic hematomas.
Patients with placental abruption commonly present with vaginal bleeding, abdominal pain, uterine tenderness, contractions, and/or fetal distress. However, the clinical presentation can be variable, and bleeding may be concealed. Our patient was intubated and sedated, limiting assessment for symptoms such as abdominal pain (1,2).
Ultrasound is one of the quickest and most readily available imaging modalities for evaluating suspected placental abruption; however, it has important limitations. The sonographic appearance of a hematoma varies with the age of the hemorrhage and may appear hyperechoic, isoechoic, or hypoechoic relative to the placenta, making diagnosis challenging (1,3). Additionally, a normal ultrasound does not exclude placental abruption (1,2). Nevertheless, identification of a retroplacental hematoma or placental separation in the appropriate clinical setting strongly supports the diagnosis and should prompt urgent obstetric consultation (1).
Management depends on the severity of the abruption, gestational age, and maternal and fetal condition, ranging from close maternal and fetal monitoring to urgent delivery when indicated (2).
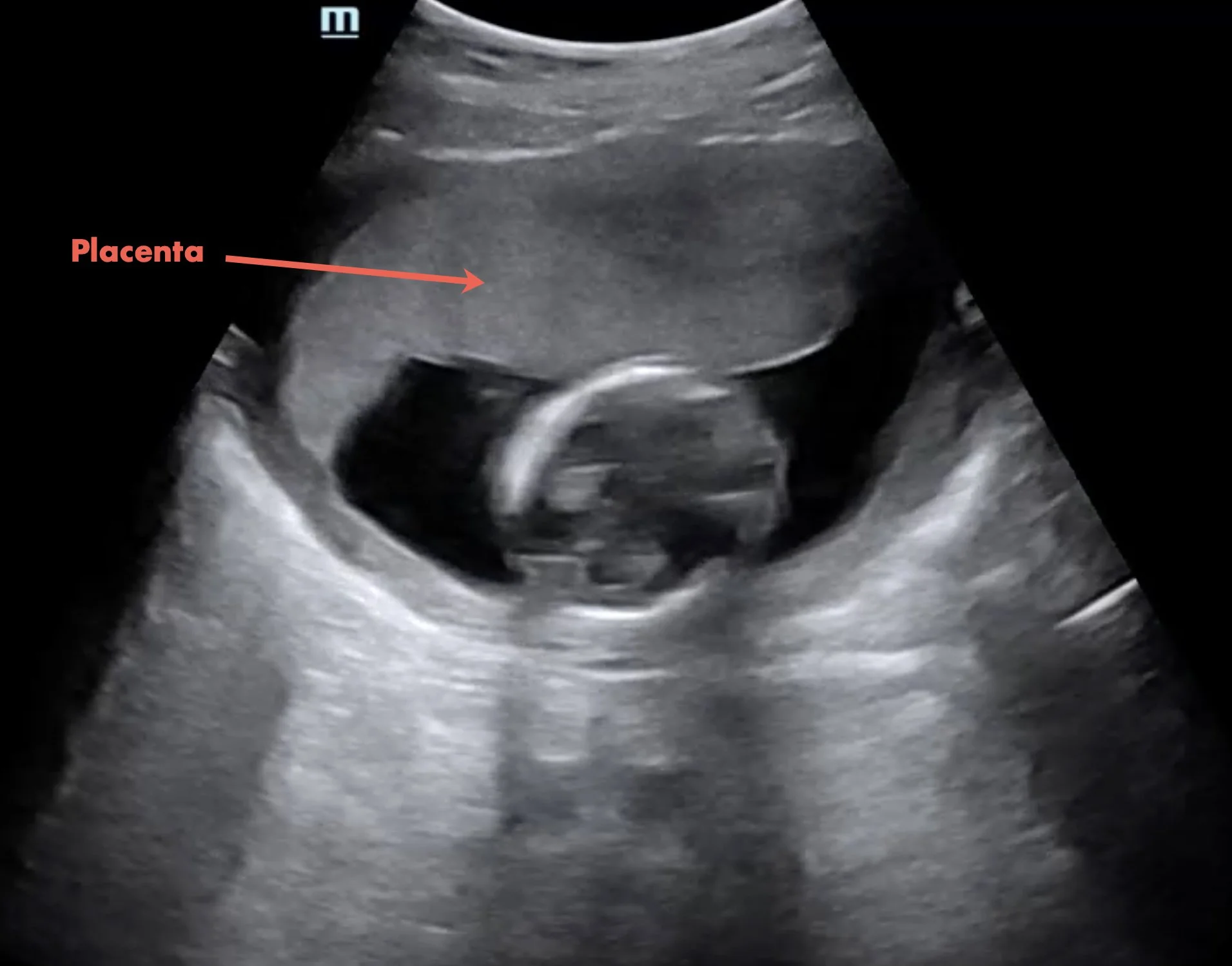
Normal placenta demonstrating homogeneous echotexture without evidence of hematoma or placental separation.
Image Acquisition
Position the patient supine for transabdominal ultrasound. If transvaginal ultrasound is performed, the patient should be placed in the dorsal lithotomy position.
Use a curvilinear transducer for transabdominal imaging and an endocavitary transducer for transvaginal imaging (2).
Identify the placenta and fan through in both sagittal and transverse planes, evaluating the entire placental margin from superior to inferior.
Assess the placenta for homogenous echotexture and smooth contour.
Use Color Doppler to evaluate suspicious collections. Normal placental tissue demonstrates vascular flow, whereas hematomas should not demonstrate internal vascularity (3,4).
Pitfalls
Depending on the age of the hemorrhage, a hematoma may appear hyperechoic, isoechoic, or hypoechoic relative to the placenta, making diagnosis challenging. Examples demonstrating the spectrum of sonographic appearances are shown below.
Acute hematomas are often isoechoic to the placenta and may therefore be difficult to detect (1,3).
The normal retroplacental venous complex is a thin hypoechoic band immediately deep to the placenta and may be mistaken for a retroplacental hematoma.
Placental thickening may represent hemorrhage but is a nonspecific finding (3).
Posterior placentas may be more difficult to evaluate sonographically than anterior placentas, further limiting the sensitivity of ultrasound for placental abruption (1,3).
Gentle pressure with the transducer may produce movement of an organized clot relative to the placenta, referred to as the "Jello sign" (5).
A normal ultrasound does not exclude placental abruption, and clinical suspicion should guide further evaluation and management (1,2).
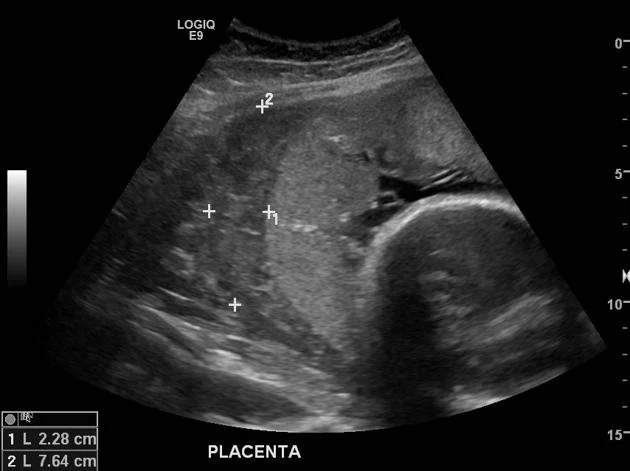
Retroplacental hematoma (7). Reproduced from Radiopaedia.org under the CC BY-NC-SA 4.0 license.

Placental abruption with isoechoic layering (8). Adapted from Radiopaedia.org under the CC BY-NC-SA 4.0 license.
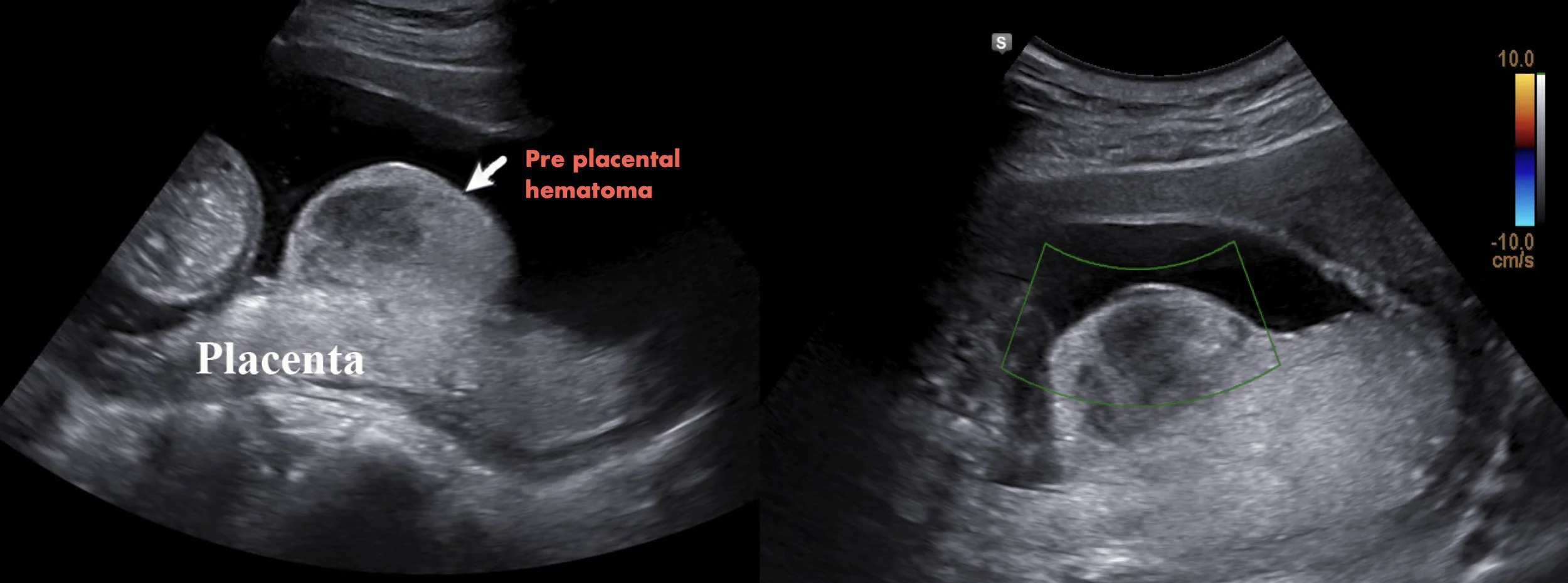
Preplacental hematoma with Color Doppler demonstrating no internal vascularity (9). Adapted from Radiopaedia.org under the CC BY-NC-SA 4.0 license.
Take-Home Points
Placental abruption is an obstetric emergency that should be considered in pregnant patients with abdominal pain, vaginal bleeding, or fetal distress.
Ultrasound is a rapid bedside adjunct for evaluating suspected placental abruption, but a normal examination does not exclude the diagnosis.
Scan through the entire placenta in multiple planes and use Color Doppler to characterize suspicious collections.
The sonographic appearance of a hematoma varies with the age of the hemorrhage, making careful image interpretation and clinical correlation essential.
AUTHORED BY: ANNA WOBSER, DO
FACULTY EDITING BY: LAUREN MCCAFFERTY, MD
References
Brandt JS, et al. Placental abruption at near-term and term gestations: Pathophysiology, epidemiology, diagnosis, and management. Am J Obstet Gynecol. 2023;228(6):603-616.
Schmidt P, Skupski DW. Placental Abruption. In: StatPearls. Treasure Island, FL: StatPearls Publishing; updated December 19, 2022. Available at: https://www.ncbi.nlm.nih.gov/books/NBK482335/
Fadl S, Moshiri M, Fligner CL, Katz DS, Dighe MK. Placental imaging: Normal appearance with review of pathologic findings. Radiographics. 2017;37(3):979-998.
Dinh V. Obstetric/OB ultrasound made easy: Step-by-step guide. POCUS 101. https://www.pocus101.com/obstetric-ob-ultrasound-made-easy-step-by-step-guide/
Oyelese Y, Ananth CV. Placental abruption. Obstet Gynecol. 2006;108(4):1005-1016.
Ali MI. Placental abruption. Case study. Radiopaedia.org. Available at: https://radiopaedia.org/cases/placental-abruption-4.
Dixon A. Placental abruption. Case study. Radiopaedia.org. Available at: https://radiopaedia.org/cases/placental-abruption.
Hacking C. Traumatic placental abruption and intra-uterine fetal death. Case study. Radiopaedia.org. Available at: https://radiopaedia.org/cases/traumatic-placental-abruption-and-intra-uterine-fetal-death.
Thapa S. Preplacental abruption. Case study. Radiopaedia.org. Available at: https://radiopaedia.org/cases/preplacental-haematoma.