Intern Ultrasound of the Month: A Case of Hydronephrosis Leading to the Diagnosis of Tubo-Ovarian Abscess
The Case
A 35-year-old female with a past medical history of recent UTI presented to the ED for two days of left-sided flank pain radiating to her groin. The day prior to presentation she developed urinary urgency, nausea, and vomiting. She denied vaginal bleeding or discharge, fevers, chills, or changes in bowel movement. She endorsed sexual activity but reported using condoms.
Her physical exam revealed a well-appearing and afebrile patient. She had left CVA tenderness and mild suprapubic tenderness with no rebound or guarding.
Renal POCUS was performed to evaluate for hydronephrosis and showed the following:
POCUS findings:
There is hydronephrosis of the left kidney. The right kidney is normal-appearing. Bladder views incidentally revealed a large complex, fluid-containing lesion in the pelvis (color doppler negative).
Case continued: Labs were significant for leukocytosis. Urine pregnancy test was negative and urinalysis did not show evidence of a UTI. CT scan showed a mixed solid and cystic lesion within the left adnexa concerning for a tubo-ovarian abscess and left-sided hydronephrosis likely due to external ureteral compression by the left adnexal mass. Transvaginal ultrasound demonstrated 8 cm tubo-ovarian abscess with dense adhesions between the sigmoid colon and bladder. The patient was started on ceftriaxone, doxycycline, and metronidazole. She was admitted to gynecology and ultimately underwent IR-guided drainage of the abscess.
Tubo-Ovarian Abscess and Pelvic Inflammatory Disease
A Quick Review of Pelvic Inflammatory Disease
Pelvic inflammatory disease (PID) is an ascending infection from the cervix to the upper reproductive tract, usually secondary to polymicrobial infection. The most common pathogens are gonorrhea and chlamydia. However, it can also be caused by H flu, strep pneumonia, group A strep, and staph aureus. It is less common during the second and third trimesters of pregnancy due to obstruction of the cervix with the mucous plug and inability of bacteria to ascend [1].
What is a tubo-ovarian abscess?
A tubo-ovarian abscess (TOA) is a fluid collection involving the ovaries or fallopian tubes that forms as a late-stage complication of PID. It is a potentially life-threatening emergency because it can rupture, leading to severe sepsis. Mortality rates have been reported as high as 5-10% when severe systemic involvement occurs [2].
Clinical Presentation
Common signs and symptoms include adnexal pain, vaginal discharge, leukocytosis, elevated inflammatory markers, or systemic signs of sepsis. Fever may be absent in 35% of patients with TOA [3]. Screening for Neisseria gonorrhea and chlamydia trachomatis are essential to obtain when diagnosing pelvic inflammatory disease or tubo-ovarian abscess but is only positive in 25% of cases [2].
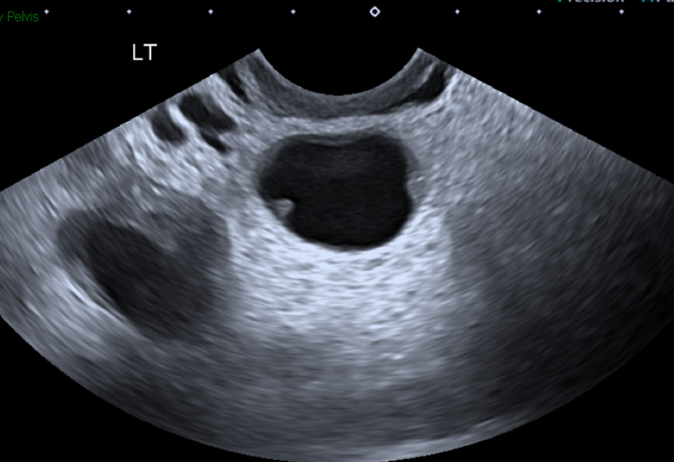
Figure 1. Tubo-ovarian abscess with cogwheel sign resulting from thickened endosalpingeal folds. [Munro]
Diagnosis
TOA is commonly diagnosed with transvaginal ultrasound and often appears as complex/cystic mass. A “cogwheel” sign may be seen, which is a thickening of the endosalpingeal folds, see Figure 1. Other imaging such as CT may be useful if concerned about other acute abdominal processes [2].
Management
IV antibiotics are effective in 70% of cases [2,4]. Ceftriaxone, doxycycline, and metronidazole is one of the recommended regimens [1]. Surgical intervention is often indicated when there are signs of TOA rupture like peritonitis or sepsis or for cases refractory to conservative management. Drainage is considered when the abscess is greater than 7 cm (1, 4].
Renal POCUS Review
Indications
Flank, back, abdominal pain especially if undifferentiated
Urinary symptoms
Difficulty voiding
Goal: evaluate for hydronephrosis
Back to Basics: How to perform a renal ultrasound [5-7]
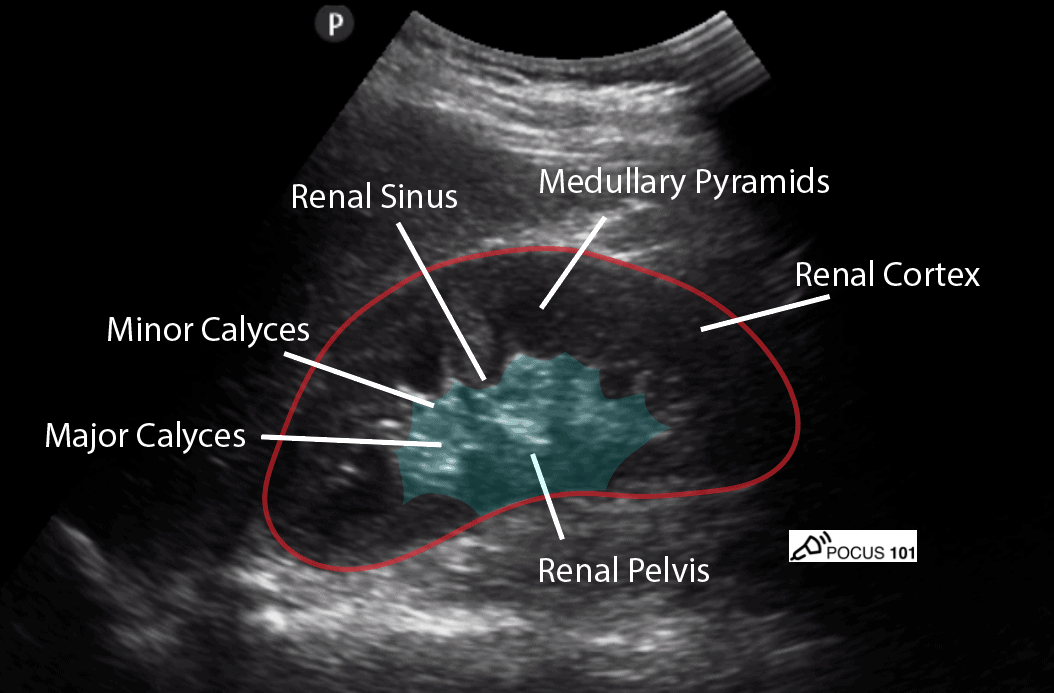
Figure 2. Sonographic appearance of normal kidney [5]
Position the patient supine with their arms above their head
Use the curvilinear probe
Evaluate each kidney followed by the bladder.
Right kidney — Obtain a longitudinal view by placing the probe on their midaxillary line on the right around the 10th rib with probe marker pointing toward the patient’s head
Identify components of the kidney (see Figure 2).
Fan through the kidney in this longitudinal view. Then rotate the probe 90 degrees to obtain the short access view and again fan through.
Evaluate primarily for hydronephrosis (and notice other abnormalities if present).
Apply color doppler to the kidney, particularly over the renal pelvis, to differentiate vasculature from hydronephrosis.
Left kidney — Place the probe on the posterior axillary line near the left flank
Similar to the right, evaluate the kidney in both longitudinal and transverse axis view, fan through in both plans, and apply the color doppler.
After evaluating both kidneys, it is necessary to obtain a bladder view — obtain a longitudinal view by placing the transducer above the pubic symphysis with the probe marker directed to the patient’s head (sagittal view)
Fan through the entire bladder.
Turn the transducer 90 degrees so the probe marker is towards the patient’s right and fan through the entire bladder in this transverse view.
When obtaining bladder views, the goal is to evaluate for urinary retention and you may find additional information that can indicate a potential cause for hydronephrosis, including a mass, clot, or large prostate.
Troubleshooting tips: if rib shadows are getting in the way, you can rotate the probe slightly (counterclockwise on the right, clockwise on the left) to better fit between the ribs. Can also ask the patient to perform deep inspiratory hold which will help bring the kidney away from rib shadows.
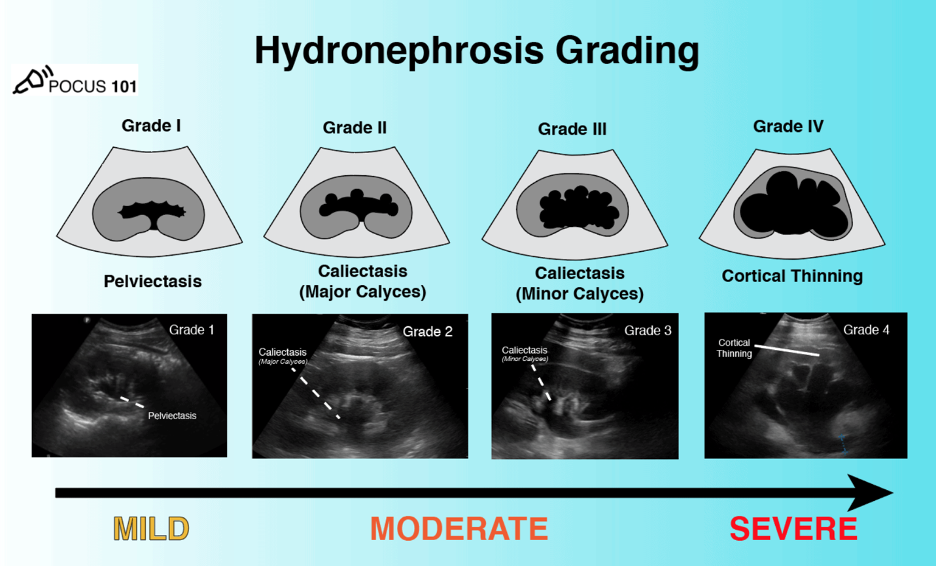
Figure 3. Grading of hydronephrosis [5]
Findings of Hydronephrosis:
Hydronephrosis results from urinary tract obstruction leading to dilation of the renal pelvis +/- ureter depending on the location of the obstruction. Therefore, the differential diagnosis can include any pathology leading to intrinsic or extrinsic obstruction, including but not limited to kidney stones, mass, clot, compression from another organ at any point in or near the genitourinary system. The presence of unilateral versus bilateral hydronephrosis can help narrow the differential, which is why it’s important to always evaluate both kidneys and the bladder, even if the patient only has unilateral symptoms [5,6]
Grading of hydronephrosis:
Hydronephrosis can be graded based on the amount of swelling in the kidney. As the grading increases, the structures in the kidney are more swollen due to the backflow. Grade 1 hydronephrosis is when the pelvis is dilated. As it progresses to grade 2, dilation also involves the major calyces. For grade 3 hydronephrosis, there is also dilation of the minor calyx. Grade 4 is indicated by cortical thinning. Determining the specific grade is less important than identifying hydronephrosis and recognizing that it’s a continuum, starting from more central structures and progressing outward as the severity increases [5].
Pitfalls
Hydronephrosis can commonly be confused with the medullary pyramids of the kidneys, as well as cysts or vascular prominence/malformation. Pyramids and renal cysts are distinct structures and tend to be more peripherally located compared to hydronephrosis which starts centrally. Vasculature can be differentiated from hydronephrosis with color doppler [5-7].
Take Home Points
POCUS is a useful tool when evaluating flank pain as well as back or abdominal/back pain
Detecting hydronephrosis can help indicate need for additional imaging
Hydronephrosis doesn’t just indicate kidney stones; it can also result from ureteral compression, outlet obstruction, dysfunctional bladder
For renal POCUS, remember to always fan through both kidneys in long and short axis, apply color doppler to differentiate hydro from prominent vasculature, and evaluate the bladder, even if pain is unilateral
Keep PID/TOA on the differential for young women of reproductive age
POST BY: DR. BROOKE OTT, PGY1
FACULTY CO-AUTHOR/EDITOR: LAUREN MCCAFFERTY, MD
References
Vieth J. Gynecologic Infections. EM:RAP CorePendium. 2023 June 1. Accessed June 2023. https://www.emrap.org/corependium/chapter/recMD39dDowygJS9k/Gynecologic-Infections#h.5q7bbzb048j5
Munro K, Gharaibeh A, Nagabushanam S, Martin C. Diagnosis and management of tubo-ovarian abscesses. The Obstetrician & Gynecologist. 2018; 20(1): 11-19.
Kairys N, Roepke C. Tubo-Ovarian Abscess. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing. 2019. https://www.ncbi.nlm.nih.gov/books/NBK448125/
Beigi RH. Management and complications of tuba-ovarian abscess. In: UpToDate. Waltham, MA. Accessed June 2023. https://www.uptodate.com/contents/management-and-complications-of-tubo-ovarian-abscess
Dinh V. Renal Ultrasound Made Easy: Step-By-Step Guide. POCUS 101. Accessed June 2023. https://www.pocus101.com/renal-ultrasound-made-easy-step-by-step-guide/
Avila J. Hydronephrosis. 5 Minute Sono. Core Ultrasound. Accessed June 2023. https://www.coreultrasound.com/hydronephrosis/
Blaivas M. Kidneys. In: Radiology Key. 2016 August 18. Accessed June 2023. https://radiologykey.com/kidneys-6/