Intern Ultrasound of the Month: "Feeling the Pressure" - A Calcaneal Avulsion Fracture
The Case
62-year-old otherwise healthy female presented to the ED following a fall. She stated she tripped and felt a pop in her right ankle with immediate pain. Has not been able to bear weight since. She reported severe pain in the posterior aspect of her ankle near the insertion of the Achilles tendon. She denied any open wounds, paresthesia, weakness, skin discoloration, or edema of the affected extremity. Also denied any other injuries.
Physical exam was notable for a positive Thompson test, inability to plantarflex her foot, and limited dorsiflexion largely limited by pain. She had tenderness to palpation over the distal Achilles/posterior calcaneus. There was focal swelling near the proximal aspect of the calcaneus and a small firm/bony-like structure was palpable just proximal to this. There was no tenting or break in the skin. No palpable tendon defect was appreciated. She was neurovascularly intact, with normal vital signs and an otherwise unremarkable physical exam.
X-rays were ordered and POCUS was performed to assess primarily for Achilles tendon tear based on her clinical assessment.





POCUS Findings
Achilles tendon appears intact
Bony fragment overlies the distal aspect of the achilles near its insertion at the calcaneus
Just distal to the bony fragment, overlying the calcaneus, is a large heterogenous fluid collection. In the setting of trauma and suspected fracture, this is concerning for hematoma.
—> Findings are concerning for calcaneal avulsion fracture (with associated hematoma) without Achilles injury
Case Continued
X-rays confirmed a posterior calcaneal avulsion fracture (type II). Podiatry was consulted who recommended emergent surgical intervention for the calcaneal fracture due to risk of necrosis. The patient underwent successful ORIF and was discharged shortly after with outpatient follow up.

Calcaneal Avulsion Fractures
Overview
Calcaneal avulsion fractures are fairly rare fractures that involve the posterosuperior aspect of the calcaneus but not the subtalar joint
Commonly result from sudden contraction of the gastrocnemius-soleus muscles, often occurring after a fall. Forced dorsiflexion pulls on the Achilles tendon, which subsequently resulting in avulsion of a bone fragment [1]
Mechanism, significance, and recommended management is based on classification
“Beak” fractures (type II) are of particular concern, as they incur significant pressure to the overlying skin (may appear as tenting) and can lead to skin necrosis if not corrected emergently [2]. In fact, over the few hours the patient was in the ED, tenting started to develop.

Classification of Avulsion Fractures & Recommended Management [2]

Classification of Avulsion Fractures [2]
Ankle Ultrasound Crash Course
POCUS can be very useful in evaluating for tendinous and osseous injury
Focused clinical questions include:
Is there evidence of tendon tear?
Is there evidence of bony abnormality (fracture, dislocation)?
Is an effusion present?
Achilles Tendon Assessment
Position the patient so that the posterior aspect of the leg is well-exposed (i.e. prone position, have foot hanging off bed, frog leg, etc).
Identify the tendon/sheath by its classic appearance — linear fibers tightly bundled within the sheath
Scan the length of the tendon from its insertion at the calcaneus to the calf muscle in both longitudinal and transverse planes.



Look for:
Disruption of the fibers — if present, suggests a tear. May appear thickened and/or irregular. Complete disruption, often with retracted edges, indicates a complete tear.
Hematoma is an indirect sign of injury, either to the tendon itself or to surrounding structures. Can use color over hematoma to evaluate for evidence of active extravasation [3-4]
Thickened tendon, hypoechoic areas, and hyperemia may be present in Achilles tendinosis [5]
Dynamic ultrasound, i.e. performing the Thompson test (or other range of motion) while directly visualizing the tendon, can augment the clinical assessment for a tendon injury [6]
A systematic review and meta-analysis found a sensitivity of 94.84%, specificity of 98.72%, positive LR of 73.98, and negative LR of 0.05 in diagnosing Achilles tendon rupture with ultrasound [3]
Cortical Assessment
Limited evidence and no well-defined protocol, but often helps to start with placing the probe over the area of maximal pain and scanning the surrounding area
Assess for disruption/irregularity in the typically smooth bony cortex. Remember that bone appears as a relatively linear hyperechoic structure with posterior shadowing. May be accompanied by hematoma formation, as demonstrated in this case

Ankle fractures on ultrasound [6]
A comprehensive POCUS assessment of the ankle/foot in patients with a positive Ottawa Ankle Rule has demonstrated a sensitivity of 100%, specificity of 99.1%, PPV 95.2%, and NPV 100%. Lateral malleolus and base of 5th metatarsal were the most commonly detected fractures [7].
Ankle Effusion Assessment
Position patient so that the sole of their foot is resting on the bed, if able
Joint effusion is best visualized with probe over anteromedial aspect of the ankle — place the probe between the medial malleolus and the anterior tibialis tendon. Can also assess anterolaterally.
Identify the tibiotalar joint and look for fluid in the immediately overlying joint space [8].
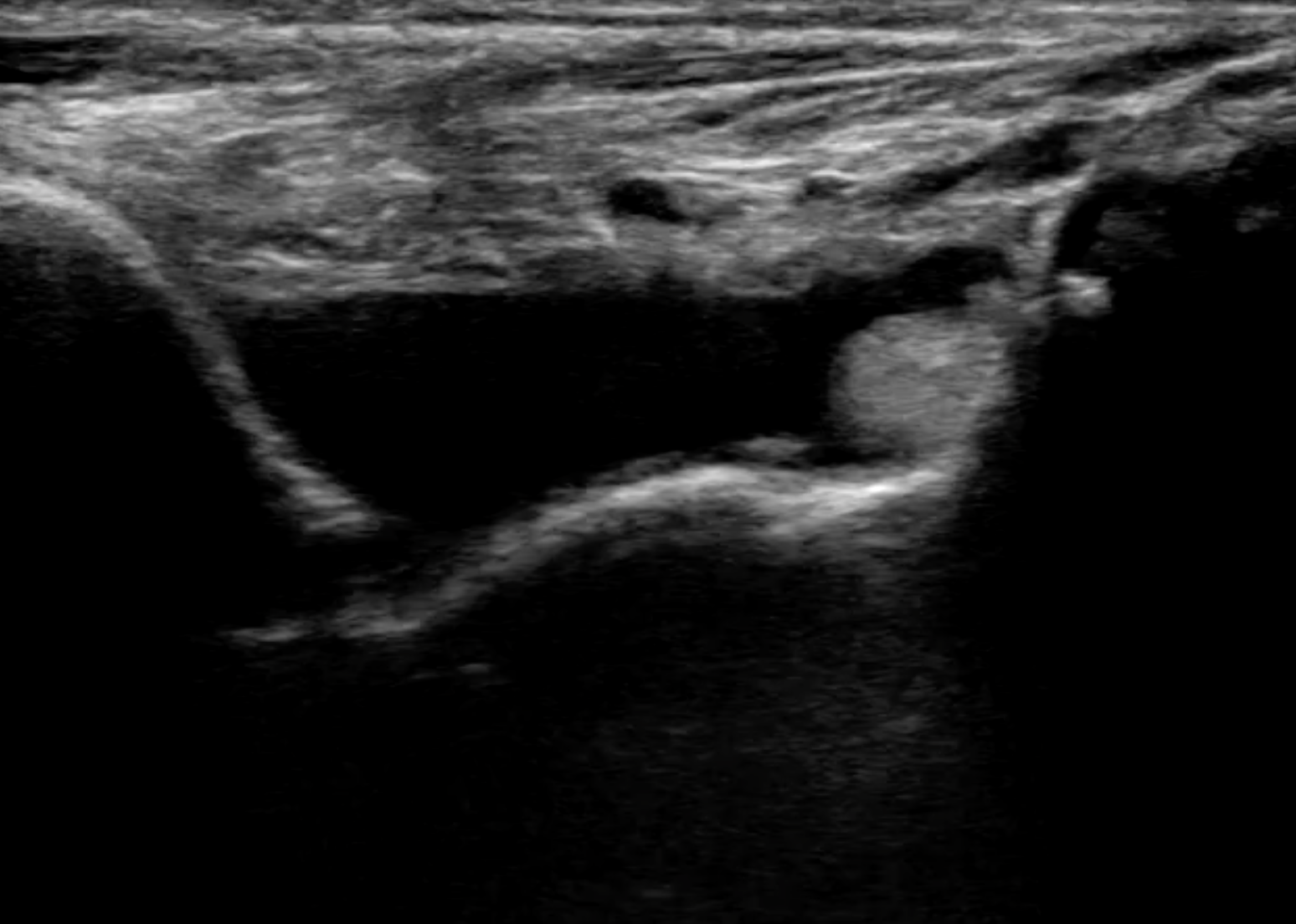
Image from: https://litfl.com/ultrasound-case-088/
Effusions can be related to trauma, infection, autoimmune/inflammatory process and indication for arthrocentesis depends heavily on clinical judgment. If arthrocentesis is indicated, consider ultrasound guidance.
Ultrasound increases success rates of arthrocentesis (96% with ultrasound vs 89% with landmarks for cadaveric models) [9]. When applied to ED patients, ultrasound guidance showed a significantly higher overall success rate (94% vs 60%), first-pass success rate, and fewer attempts [10].
*These are some of the more common assessments and are not comprehensive. For additional ligamentous/tendinous injuries, ultrasound has shown similar sensitivity as MRI [11]
Take Home Points
Calcaneal avulsion fractures warrant a prompt skin assessment of the posterior ankle/heel and may require emergent surgical intervention.
POCUS can efficiently evaluate various anatomical aspects of the ankle/foot including tendons, bony structures, surrounding soft tissue, vessels, etc.
Ultrasound has high diagnostic accuracy for ankle/foot injuries including tendon tears, fractures, and effusions
Compared to x-ray and other imaging modalities, POCUS offers the advantages of dynamic imaging and clinical correlation while not incurring radiation exposure or extensive amounts of time
AUTHORED BY: DR. JUAN VALDES INFANTE (R1)
FACULTY CO-AUTHOR/EDITOR: LAUREN MCCAFFERTY, MD
References
Hess M, Booth B, Laughlin RT. Calcaneal avulsion fractures: complications from delayed treatment. Am J Emerg Med. 2008; 26(2): 254.e1-254.e4
Lee SM, Huh SW, Chung JW, Kim DW, Kim YJ, Rhee SK. Avulsion fracture of the calcaneal tuberosity: classification and its characteristics. J Clin Ortho Surg. 2012; 4(2):134-8.
Aminlari A, Stone J, McKee R, Subramony R, Nadolski A, Tolia V, Hayden SR. Diagnosing Achilles Tendon Rupture with Ultrasound in Patients Treated Surgically: A Systematic Review and Meta-Analysis. J Emerg Med. 2021; 61(5): 558-567.
Adhikari S, Marx J, Crum T. Point-of-care ultrasound diagnosis of acute Achilles tendon rupture in the ED. Am J Emerg Med; 2012; 30(4): 634.e 3-4.
Mitchell AWM, Lee JC, Healy JC. Aspects of Current Management: The use of ultrasound in the assessment and treatment of Achilles tendinosis. J Bone Joint Surg [Br]. 2009; 11:91–1405.
Griffin M, Olson K, Heckmann N, Charlton TP. Realtime Achilles ultrasound Thompson (RAUT) test for the evaluation and diagnosis of acute Achilles tendon ruptures. Foot Ankle Int. 2017;38:36–40.
Ekinci S, Polat O, Günalp M, Demirkan A, Koca A. The accuracy of ultrasound evaluation in foot and ankle trauma. Am J Emerg Med. 2013; 31: 1551-1555.
Nagdev A. Using Point-of-Care Ultrasound to Evaluate and Aspirate Ankle Infections. ACEP Now. Published January 21, 2020. <https://www.acepnow.com/article/using-point-of-care-ultrasound-to-evaluate-and-aspirate-ankle-infections/> [Accessed 10 April 2022].
Beron K, Abdi A, Menchine M, Mailhot T, Kang T, Seif D, Chilstrom M. Success of ultrasound-guided versus landmark-guided arthrocentesis of hip, ankle, and wrist in a cadaver model. Am J Emerg Med. 2017; 35(2): 240-244.
Gibbons RC, Zanaboni A, Genninger J, Costantino TG. Ultrasound-versus landmark-guided medium-sized joint arthrocentesis: A randomized clinical trial. Acad Emerg Med. 2022; 29(2), 159–163.
Margetić P, Pavić R. Comparative Assessment of the Acute Ankle Injury by Ultrasound and Magnetic Resonance. Collegium antropologicum. 2012; 36(2): 605-610.