Intern Ultrasound of the Month: IVC Thrombus Leading to Diagnosis of Cancer
-Dr. Haley Wartman, PGY1
The Case
58 yo female with past medical history of hypertension, diabetes, asthma, osteoarthritis presented to the ED for a few days of nausea, poor appetite, and vague abdominal discomfort worse in right mid abdomen. On further questioning, she also reported intermittent hematuria for 3 months and 10-15 lb weight loss over several months prior to this. ROS otherwise negative.
On arrival to the ED, her vitals were within normal limits. She was somewhat uncomfortable appearing but nontoxic and in no acute distress. She had mild diffuse right sided abdominal tenderness. No signs of peritonitis. No CVA tenderness. She was neurovascularly intact.
POCUS of the aorta and renal ultrasound were performed and significant for the following:




POCUS findings: While the aorta & kidneys were both unremarkable — no AAA/dissection or hydronephrosis — a well-circumscribed echogenic mass without internal flow is seen adjacent to the aorta just right of midline (relative to the patient) and extending toward patient’s left. It appears to extend from the IVC, which raises suspicion for IVC thrombus (vs mass).

Case Continued: The patient initially declined CT and wanted to go home and follow up outpatient. However, after discussion of concerning ultrasound findings, she was agreeable to staying for CT. CT showed extensive metastatic disease (not previously known) with large thrombus in the IVC and left renal vein. She had a nonspecific retroperitoneal mass but no obvious primary malignancy. Her labs were within normal limits aside from hematuria. She was started on a heparin drip and vascular surgery was consulted. She was admitted to the hospital for oncologic workup and management. Her thrombus was determined to be tumor thrombus so anticoagulation was discontinued. She was ultimately diagnosed with high grade sarcoma and is in the planning stages for treatment.

Tumor Thrombus
Tumor thrombus = intravascular metastatic tumor with thrombotic elements
Differentiate from “bland thrombus” = thrombus free of neoplastic cells
Most commonly seen with renal cell carcinoma, Wilm’s tumor, adrenal cortical carcinoma, hepatocellular carcinoma, retroperitoneal sarcoma, leiomyosarcoma but can occur with other types as well [1-4].
IVC involvement = worse prognosis. Factors affecting outcome include: IVC wall invasion, height of tumor thrombus, primary tumor location, presence of bland thrombus, presence of collateral circulation [2, 5]
Presentation can be vague and highly variable
May include varicoceles, lower extremity swelling/pain, abdominal/flank/back pain, scrotal swelling, urinary symptoms, cardiac dysfunction, Budd Chiari syndrome [1, 6]
Imaging plays key role in diagnosis
CT or MRI are best for assessing local & distant extension of tumor, staging, etc. [2]
Doppler sonography, particularly contrast enhanced, shown to have high diagnostic accuracy in identifying IVC wall invasion and differentiating bland and tumor thrombus [5, 7-9]
While certainly not comprehensive, POCUS can aid in providing a quick diagnosis of IVC thrombus (tumor or bland) &, thus, expedite additional imaging and appropriate management [10-12]
Consider anticoagulation until bland thrombus is ruled out as there is increased risk for PE [6].
Surgical resection is often indicated to reduce poor outcomes but depends on type and extent of thrombus and malignancy [3, 4].
POCUS Evaluation of the IVC
IVC evaluation is usually more for volume status rather than thrombus. The latter is often found incidentally when performing other POCUS studies. The focus here will be on IVC location/identification & discussion of thrombus. Volume assessment is a separate, extensive discussion on its own and isn’t covered here.
Technique [13-15]
Probe: low frequency (curvilinear or phased array)
Identify the IVC in any of the following views
Subcostal sagittal view (junction of right atrium/IVC) — typical view for volume assessment
Place transducer in subxiphoid region with probe marker toward either the patient’s feet (more conventional abdominal imaging orientation with cephalad structures on left of screen and caudal structures on the right ) or head — either are acceptable
Can start with subxiphoid cardiac view. Center the right atrium on the screen and rotate probe 90 degrees.
Probe should be relatively perpendicular to the skin, perhaps slightly pointing toward the patient’s right. Typically doesn’t require much pressure (certainly less than a subxiphoid cardiac view)
If not visualizing the heart, may need to slide the probe more superiorly until this comes into view
Longitudinal IVC View (abdomen)
Sliding the probe more caudally, you can visualize the more distal aspects of the IVC. Just make sure you’re looking at the IVC, not the aorta (see below)

Transverse IVC/Aorta View (standard aorta views but focusing on IVC)
From the longitudinal view, rotate probe 90 degrees so the probe marker is pointing toward the patient’s right
Identify the vertebral shadow. Look for the IVC and aorta lying just above. IVC is always to the patient right and aorta to the left
Keep these structures in view as you slide the probe caudally
May need to apply graded compression to displace bowel gas

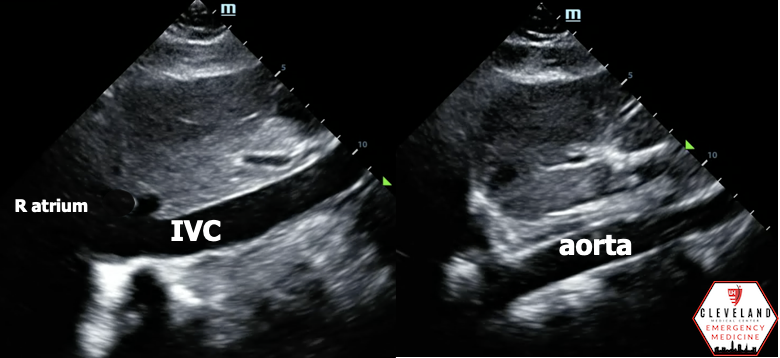
Differentiate IVC from aorta
IVC:
Thinner walls
Travels through the liver; parenchyma will be directly adjacent to the vessel* (see images below)
Drains into the right atrium*
Hepatic veins drain into it* (hepatic confluence)
May see respiratory variation (collapsibility with inspiration)
Lacks pulsatile flow on pulse wave doppler
Won’t have sequential anterior branches in the abdomen like the aorta does (i.e. celiac, SMA)
*= seen in the subcostal sagittal view

IVC Thrombus
Look for thrombus in vessel — echogenic material within the lumen
Non compressible
Can result in complete occlusion
May or may not result in dilation/enlargement of vessel
Partial or complete absence of flow in the vessel lumen with color doppler
Monophasic waveform/decreased respiratory variation with PW doppler
Tumor thrombus often appears similar to bland thrombus but features suggestive of tumor thrombus include:
Internal vascularity
Adjacent tumor
Invasion of the wall [5, 7-9]

The Evidence
The evidence for POCUS assessment/detection of IVC thrombus is sparse — Includes one case report of tumor thrombus [12] and two case reports of bland tumor thrombus [10-11] diagnosed by POCUS in the ED
One study showed color doppler sonography to be 100% accurate in assessing presence and extent of IVC tumor thrombus [8]
Ultrasound, particularly contrast-enhanced, has been shown to have some diagnostic advantages over CT/MRI [7], particularly in differentiating bland from tumor thrombus [5, 9] However, it also has its disadvantages (including operator dependence, artifacts, more limited assessment of extent of disease) and has also not been extensively compared directly with CT/MRI.
Take Home Points
POCUS can help in identifying IVC thrombus. It may not be a typical indication but pattern recognition is important!
Not all IVC thrombi are the same (tumor vs bland)
Limited published evidence in diagnosing IVC thrombus by POCUS (or ultrasound in general), but what is out there is supportive!
References
Quencer KB, Friedman T, Sheth R, Oklu R. Tumor thrombus: Incidence, imaging, prognosis and treatment. Cardiovasc Diagn Ther. 2017;7(Suppl 3):S165-S177. doi:10.21037/cdt.2017.09.16.
Molina M, Schiappacasse G, Labra A. Tumours that invade the inferior vena cava: An illustrative review of the main imaging features on computed tomography and magnetic resonance. Rev Chil Radiol. 2016;22(1):39-46.
Tsuji Y, Goto A, Hara I, et al. Renal cell carcinoma with extension of tumor thrombus into the vena cava: Surgical strategy and prognosis. J Vasc Surg. 2001;33(4):789-796.
Hamblen V. Sonographic Evaluation of Inferior Vena Cava Tumor Thrombus in Renal Cell Carcinoma: A Case Study of a Rare Condition. J Diagnostic Med Sonogr. 2018;34(5):375-382.
Li QY, Li N, Huang QB, et al. Contrast-enhanced ultrasound in detecting wall invasion and differentiating bland from tumor thrombus during robot-assisted inferior vena cava thrombectomy for renal cell carcinoma. Cancer Imaging. 2019;19(1):1-11.
Hollingsworth CM, Mead T. Inferior Vena Caval Thrombosis. [Updated 2020 Jul 10]. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2021.
Khan AR. Anwar K, Fatima N, Khan SF. Comparison of CT scan and colour flow Doppler ultrasound in Detecting venous tumour thormbous in renal cell carcinoma. J Ayub Med Coll Abbottabad. 2008; 20(3):47-50.
Habboub HK, Abu-Yousef MM, Williams RD, See WA, Schweiger GD. Accuracy of color Doppler sonography in assessing venous thrombus extension in renal cell carcinoma. Am J Roentgenol. 1997;168(1):267-271.
Li Q. Wang Z, Ma X, Tang J, Luo Y. Diagnostic accuracy of contrast-enhanced ultrasound for detecting bland thrombus from inferior vena cava tumor thrombus in patients with renal cell carcinoma. Int Braz J Urol. 2020; 46 (1): 92-100.
Lahham S, Tsai L, Wilson SP, Barton ED, et al. Thrombosis of inferior vena cava diagnosed using point-of-care ultrasound after pediatric near-syncope. J Emerg Med. 2016; 51(4): E89-91
Yanuck J, Ghanem G, Lahham S. Detection of Inferior Vena Cava Thrombosis Extending into the Right Atrium Using Point-of-care Ultrasound. Clin Pract Cases Emerg Med. 2019;3(1):67-68.
Toy J, Garrett A, Liu Y. Man with bilateral leg swelling. Clin Pract Cases Emerg Med. 2019; 3(4): 451-452.
Ma OJ, Mateer JR, Reardon RF, & Joing S. (2014). Ma and Mateer's Emergency Ultrasound. New York, NY: McGraw-Hill Education.
Gibbons RC, Kane D. IVC and Fluid Responsiveness. Excerpt From: Resa E. Lewiss. “Practical Guide to Critical Ultrasound, Volume 1.” American College of Emergency Physicians, 2018. Apple Books.
Koratala, A. Inferior Vena Cava POCUS: The Basics of Image Acquisition. Renal Fellow Network. 20 March 2020.